.gif "IP Gear")















- Joined
- Apr 22, 2011
- Messages
- 43
Hello all. Wanted to make a quick post and provide updates regarding the protocol I'm using to restore my HPTA after years of steroid use. I'm 28, started using AAS at 20. Did a couple of cycles, stayed on for around a year I think, went off for a year or so, went back on for a few years straight, tried to post cycle at the end of '09 but just ended up getting back on, and now here I am.
I've only been running ~250mg Test-E/week for the past couple months, just getting my body used to a somewhat normal T level.
I am now 5 weeks into what I feel is a very promising post cycle protocol.
Here it is:
Week 1-15 HCG @ 1666IU 2x/week
Week 1-10 HMG @ 37.5IU 2x/week
Week 1-20 clomiphene citrate @ 50mg 2x/day
Week 1-15 tamoxifen citrate @ 20mg/day
Week 1-6 Methandrostenolone @ 10mg/day in the morning
Week 1-15 exemestane @ 25mg/day
Week 6: triptorelin acetate @ 100mcg
Week 1-6 Test-E @ 100mg/week
Week 7-12 taper Test-E by 20mg/week
Here's my thinking:
1. I need to get the gonads going again. I do this by stimulating them with LH & FSH analogs.
2. I need to get my hypothalamic-pituitary axis back in line. I do this with clomiphene, tamoxifen, exemestane, and triptorelin. Reduce estrogen, stimulate gonadotrope release.
3. There isn't going to be an instantaneous recovery, so some exogenous T is required to keep me from feeling like shit. I am basing my post-cycle T usage off of Prisoner's Test-Taper protocol.
I felt like shit the first few weeks of this, depressed and crying and shit (gay I know). Dick was all shriveled up and never got hard. But I'm also living in a shitty place right now and dealing with a fucked up girl situation so that can't help.
I'm actually feeling pretty great after 5 weeks, and I expect to continue to feel better as my body acclimates to mere mortal levels of T.
Sex drive isn't what it used to be on high levels of T and living with a hot girlfriend, but I feel it coming back. I'm getting raging morning woods again and am actually able to successfully jack it now. I'm blowing huge loads too, way more than I ever did on AAS, I take that as a good sign.
Sorry if some of that was TMI for some of the more faint-hearted members, but these are all things we deal with when trying to kick the steroid habit.
My reasons for discontinuing steroid usage are multiple. My lipid profile was fucked all to hell and I really started getting scared I was developing CAD and was going to die. Also, I was just damn tired of being dependent on something. I want to let my body take control again and not have to worry about sticking myself every week and sourcing more juice and who should I tell and all that bullshit that comes along with this stuff. No doubt I had an awesome time while on and even won a contest, but I'm moving on.
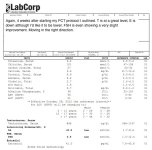
I will be getting monthly labs in addition to the ones I have already had. All results will be posted so others can follow my recovery.
Check out my attached labs.
I've only been running ~250mg Test-E/week for the past couple months, just getting my body used to a somewhat normal T level.
I am now 5 weeks into what I feel is a very promising post cycle protocol.
Here it is:
Week 1-15 HCG @ 1666IU 2x/week
Week 1-10 HMG @ 37.5IU 2x/week
Week 1-20 clomiphene citrate @ 50mg 2x/day
Week 1-15 tamoxifen citrate @ 20mg/day
Week 1-6 Methandrostenolone @ 10mg/day in the morning
Week 1-15 exemestane @ 25mg/day
Week 6: triptorelin acetate @ 100mcg
Week 1-6 Test-E @ 100mg/week
Week 7-12 taper Test-E by 20mg/week
Here's my thinking:
1. I need to get the gonads going again. I do this by stimulating them with LH & FSH analogs.
2. I need to get my hypothalamic-pituitary axis back in line. I do this with clomiphene, tamoxifen, exemestane, and triptorelin. Reduce estrogen, stimulate gonadotrope release.
3. There isn't going to be an instantaneous recovery, so some exogenous T is required to keep me from feeling like shit. I am basing my post-cycle T usage off of Prisoner's Test-Taper protocol.
I felt like shit the first few weeks of this, depressed and crying and shit (gay I know). Dick was all shriveled up and never got hard. But I'm also living in a shitty place right now and dealing with a fucked up girl situation so that can't help.
I'm actually feeling pretty great after 5 weeks, and I expect to continue to feel better as my body acclimates to mere mortal levels of T.
Sex drive isn't what it used to be on high levels of T and living with a hot girlfriend, but I feel it coming back. I'm getting raging morning woods again and am actually able to successfully jack it now. I'm blowing huge loads too, way more than I ever did on AAS, I take that as a good sign.
Sorry if some of that was TMI for some of the more faint-hearted members, but these are all things we deal with when trying to kick the steroid habit.
My reasons for discontinuing steroid usage are multiple. My lipid profile was fucked all to hell and I really started getting scared I was developing CAD and was going to die. Also, I was just damn tired of being dependent on something. I want to let my body take control again and not have to worry about sticking myself every week and sourcing more juice and who should I tell and all that bullshit that comes along with this stuff. No doubt I had an awesome time while on and even won a contest, but I'm moving on.
I will be getting monthly labs in addition to the ones I have already had. All results will be posted so others can follow my recovery.
Check out my attached labs.
Attachments





Last edited: