
- Joined
- Sep 21, 2010
- Messages
- 4,067
Maybe the IGF boosts intratesticular e2? I know IGF from GH keeps balls bigger just my experience.

































.gif "IP Gear")















Do you have a reference? All information ive seen on aromasin states that maximum estradiol suppression happens at 12hrs and takes 3-6 days to return to baseline.Also, exemestane has a halflife of 9 hours in men, I'd dose it more often than 2x per week.
 academic.oup.com
academic.oup.com
Almost impossible for e2 to be so high with normal test levels, since all e2 comes from aromatization of test, definitely get the sensitive/ultrasensitive test (this means they use a MS/LC testing method)

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
Do you have a reference? All information ive seen on aromasin states that maximum estradiol suppression happens at 12hrs and takes 3-6 days to return to baseline.
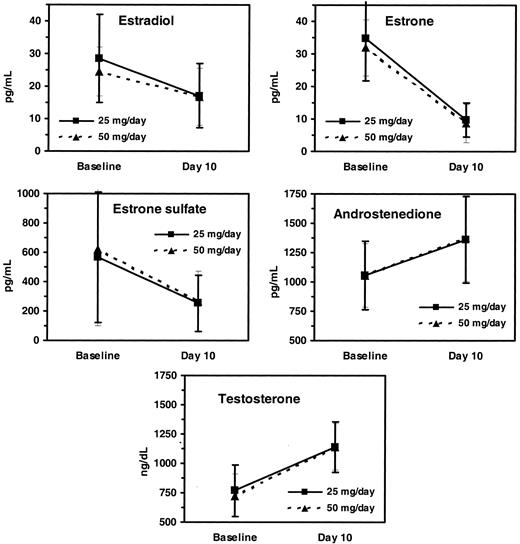
Pharmacokinetics and Dose Finding of a Potent Aromatase Inhibitor, Aromasin (Exemestane), in Young Males
Abstract. Suppression of estrogen, via estrogen receptor or aromatase blockade, is being investigated in the treatment of different conditions. Exemestane (Arom
I maintain the belief that shbg has an important role in estrogen conversion. There's several things at play but I think shbg is too often overlooked.
I'm curious as to why his shbg is so low. In a normal person, that is indicative of insulin resistance. My shbg was a 22 when last tested and I seem to need my estradiol really low or I'll balloon up, lose my appetite, energy, sex drive, strength. I dont feel good with estradiol between 20-30.
The terminal half-life was 8.9 h.
Please enlighten me on other pathways for the production of estradiol.
Also, I'm not saying use other AIs, why not just dose the exemestane more frequently? I personally break my tabs into quarters and dose ED or EOD.

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Every time I used LR3 IGF I was more sensitive to hCG and lowered my doses of it.Maybe the IGF boosts intratesticular e2? I know IGF from GH keeps balls bigger just my experience.

ALA, SDA ≠ DHA, EPAWhy not use organic hemp oil for omegas? The ocean is polluted AF in case you haven't got the memo
DHA and EPA are non-essential meaning if you consume enough omega 3 oil your body will produce them. You're welcome.ALA, SDA ≠ DHA, EPA
DHA and EPA are non-essential meaning if you consume enough omega 3 oil your body will produce them. You're welcome.
The parent fatty acid ALA (18:3n-3), found in vegetable oils such as flaxseed or rapeseed oil, is used by the human organism partly as a source of energy, partly as a precursor of the metabolites, but the degree of conversion appears to be unreliable and restricted. More specifically, most studies in humans have shown that whereas a certain, though restricted, conversion of high doses of ALA to EPA occurs, conversion to DHA is severely restricted.
[...]
These findings indicate that future attention will have to focus on the adequate provision of DHA which can reliably be achieved only with the supply of the preformed long-chain metabolite.
pubmed.ncbi.nlm.nih.gov
Human beings are poor DHA synthesizers, possibly because of their LC(n-3)P-abundant ancient diet. Dietary changes in the past century have lowered the (n-3) status to a current state of subclinical deficiency that is epidemiologically related to CVD, inflammatory disorders, mental and psychiatric diseases and suboptimal neurodevelopment. The strongest evidence comes from randomized controlled trials with LC(n-3)P, showing reduced mortality from CVD, improved neonatal neurodevelopment, and lower blood pressure in later life. With these studies as evidence, we conclude that DHA is likely to be essential.
 academic.oup.com
academic.oup.com
The FAO and EFSA suggest a long-chain omega-3 fat (EPA and DHA) intake of 250 milligrams per day for adults. Vegans consume almost none of these fats from natural sources. It is possible to supplement a vegan diet with EPA and DHA from microalgae, which may be a particularly important consideration for infants and those who are pregnant or breastfeeding, due to the role of omega-3 fat in brain health. However, we require more research into how supplementation affects the health of vegans.

You should try non flush niacin at 1-1,5 gr per day after a tren cycle. It works wonders at raising HDL. You have to watch out and don't overuse it because it raises liver enzymes. Nothing to worry about if you stopped it and if you don't drink and take other orals. Give it a try. I always use it with the addition of 3gr of pharma fish oil
after all cycles ,for 3-4 weeks, do some blood tests and all is in range. Not on cycle because it's waste.
High IGF-1 and IGFBP3 = increased estradiol in ageing men
Associations of plasma IGF1, IGFBP3 and estradiol with leucocyte telomere length, a marker of biological age, in men - PubMed
Higher IGF1 and IGFBP3 are independently associated with longer telomeres in older men. Additive associations of higher IGF1 and higher estradiol with telomere length are present. Further studies are needed to determine whether these hormonal exposures cooperate to slow biological aging.
To test the hypothesis that insulin-like growth factor (IGF-I) is required for the in vivo development of testicular Leydig cell function, either recombinant human GH [(hGH) (1.5 micrograms/g BW) or recombinant IGF-I (1 microgram/g BW) was injected three times daily into immature Snell dwarf mice (dw/dw) and into phenotypically normal control (Dw/-) for 7 days. In dw/dw mice hGH enhanced significantly body, liver, kidney, and testicular weight. In addition, hGH increased testicular LH receptors and the acute steroidogenic response to human CG, but there was no significant effect on basal plasma testosterone or plasma LH levels. The effects of IGF-I in body and kidney weight were less pronounced than those produced by hGH, but its effects on testicular weight and LH receptors, as well as on the acute steroidogenic response to human CG, were similar to that observed after hGH treatment. In Dw/- mice hGH had no effect on either body or organ weight or on testicular function, despite the fact that it induced a significant increase in plasma IGF-I levels. These results indicated that IGF-I is able to induce the maturation of Leydig cell function and that the effects of hGH on the testis are probably mediated by IGF-I. They also suggest that the delayed puberty associated with GH deficiency or resistance is most likely related to an IGF-I deficiency.
pubmed.ncbi.nlm.nih.gov
Objective: To evaluate the effect of growth hormone (GH) therapy on pubertal onset, pubertal pace, adult testicular function, and adrenarche in boys with non-GH-deficient short stature.
Study design: Randomized, double-blind, placebo-controlled trial. GH (0.074 mg/kg, subcutaneously, 3 times per week) or placebo treatment was initiated in prepubertal or early pubertal boys and continued until near final height was reached (n = 49). Statistical significance was assessed by survival analysis, repeated-measures analysis of variance, and Student t test.
Results: GH therapy did not affect the age at pubertal onset, defined either by testicular volume >4 mL or by testosterone concentration >1.0 nmol/L (30 ng/dL). GH treatment also did not affect the pace of puberty, defined either by the rate of change in testicular volume or testosterone concentration during the 4 years after pubertal onset. In boys followed up to age > or =16 years during the study, there were no significant differences in final testicular volume or in plasma testosterone, luteinizing hormone, or follicle-stimulating hormone concentrations. The pace of adrenarche, assessed by change in dehydroepiandrosterone sulfate levels over time, also did not differ significantly between the GH and placebo groups.
Conclusion: Our findings suggest that GH treatment does not cause testicular damage, alter the onset or pace of puberty, or alter the pace of adrenarche in boys with non-GH-deficient short stature.

 www.sciencedirect.com
www.sciencedirect.com
Aim: To study the influence of growth hormone (GH) treatment on the initiation and progression of puberty in short children.
Methods: This prospective, randomized, controlled study included 124 short children (33 girls) who received GH treatment (Genotropin®; Pfizer Inc.) from a mean age of 11 years until near adult height [intent-to-treat (ITT) population]. Children were randomized into three groups: controls (n = 33), GH 33 μg/kg/day (n = 34) or GH 67 μg/kg/day (n = 57). Prepubertal children at study start constituted the per-protocol (PP) population (n = 101). Auxological measurements were made and puberty was staged every 3 months. Serum sex-steroid concentrations were assessed every 6 months.
Results: No significant differences were found between the groups, of both PP and ITT populations, in time elapsed from start of treatment until either onset of puberty, age at start of puberty or age at final pubertal maturation in either sex. In the ITT population, pubertal duration was significantly longer in GH-treated girls, and maximum mean testicular volume was significantly greater in GH-treated boys than controls, but there were no differences in testosterone levels between the groups.
Conclusion: GH treatment did not influence age at onset of puberty and did not accelerate pubertal development. In boys, GH treatment appeared to increase testicular volume.
pubmed.ncbi.nlm.nih.gov























