
©ALL CONTENT OF THIS WEBSITE IS COPYRIGHTED AND CANNOT BE REPRODUCED WITHOUT THE ADMINISTRATORS CONSENT 2002-2024


























You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.







.gif "IP Gear")















Thick blood
- Thread starter aphextwin
- Start date
If I'm not mistaken, I though I read Dante saying something about IP-6 helping control Hematacrit levels.....I might be completely off base. If he sees this, maybe he can add his input, but he's a busy guy.
Stewie??
Stewie??
- Joined
- Jan 15, 2011
- Messages
- 13,119
If I'm not mistaken, I though I read Dante saying something about IP-6 helping control Hematacrit levels.....I might be completely off base. If he sees this, maybe he can add his input, but he's a busy guy.
Stewie??
Look for Dante's IG post about it. He said he sees it lower hematocrit by 1-3 points in most people. Worth nothing it can decrease ferritin though, so be careful.
- Joined
- Jun 12, 2003
- Messages
- 4,665
Btw, the same Dr. John Crisler who had the heart attack was also in the "high hematocrit is okay" team.He was extremely fit and active, regularly doing cardio, controlling his BP, etc. Access to the best medicine, advice from his peers, etc.
Hematocrit is associated with carotid atherosclerosis in men but not in women.
https://www.ncbi.nlm.nih.gov/m/pubmed/12826926/
Atherosclerosis is another major factor in heart attack/stroke risk. Suggesting that high hematocrit is okay is dangerous.
That is absolutely incorrect. He had his heart attack i believe in March of 2016 when he recommended phlebotomizing and absolutely cut off anyone off of TRT with a hematocrit of 55.....so here we are with repeated phlebotomy again maybe a culprit and not a cure......it was only later after Dr Rouzier came out with his erythrocytosis/testosterone scenario that Dr Crisler (AFTER HIS HEART ATTACK NOT BEFORE when he believed in phlebotomies) stated:
"I wish you had all seen the incredible 90 minute lecture my old pal Dr Neal Rouzier just gave at AMMG. There is absolutely no reason to perform therapeutic phlebotomies in men on TRT whose H/H rises above 18/55, as long as platelets have not risen too high. Based upon irrefutable evidence-based medicine, I am changing my practices."
I personally am on the fence about the whole subject, worried much less about high hematocrit than if you asked me 10 years ago....I dont know the answer exactly, nobody is absolutely sure and alot of it is theory and guesswork by many elite minds right now....but i do know this.....there have been 1000's upon 1000's of bodybuilders competing in colorado for decades where it has been shown in many high altitude areas the average hematocrit is 50-52 and hemoglobin is 17-18...thats the AVERAGE HCT with people not even bodybuilders. Now think of all those 1000's upon 1000's of enhanced bodybuilders with high hematocrit dehydrated from training/cardio/prep what have you.....compound that dehydration with diuretics and curbing back water intake before colorado shows....do you see anyone clotting out? Nobody is clotting out at contests or in their gyms in colorado.
Last edited:
Seem to be a good amount of professional cyclists that have had clots and some died from. I hope someday we understand better what the relationship is.
Probably the gallons of EPO they use bro lol
XstarchildX
Banned
- Joined
- Oct 23, 2015
- Messages
- 1,538
I am just theorizing here, but I think a lot of that has to do with blood doping in general. When you ADD blood volume, it will automatically increase platelet count due to having more platelets. That is a primary risk for clotting. Combine that with a long ride and likely lower than optimal water levels due to excretion of bodily fluids through sweating, and you could compound the risk.Seem to be a good amount of professional cyclists that have had clots and some died from. I hope someday we understand better what the relationship is.
Just spit balling here, so I could be way off the mark.
- Joined
- Jan 15, 2011
- Messages
- 13,119
I am just theorizing here, but I think a lot of that has to do with blood doping in general. When you ADD blood volume, it will automatically increase platelet count due to having more platelets. That is a primary risk for clotting. Combine that with a long ride and likely lower than optimal water levels due to excretion of bodily fluids through sweating, and you could compound the risk.
Just spit balling here, so I could be way off the mark.
So I was wondering whether EPO increased platelets and found this
**broken link removed**
"In summary, we showed that EPO markedly enhances platelet and endothelial activation in humans. Thus, we postulate that a patient-oriented approach to the use of EPO entails its administration not only to patients who are likely to respond to EPO but also to anemic patients, who additionally benefit from platelet activation. Whether heightened platelet reactivity and endothelial activation may increase the risk of thromboembolism warrants further investigation."
Here is another
https://www.ncbi.nlm.nih.gov/pubmed/10366799
"A 10% to 20% increase in platelet counts was observed in both EPO groups on day 5. In the placebo group, platelets increased only several days after the first phlebotomy."
So that is interesting because the vast majority of us on TRT/AAS generally do not seem to get increased platelets. So wouldn't that mean the mechanism IS different between TRT/AAS and taking EPO?? I am not sure we face the same risks those cyclists did.
Last edited:
- Joined
- Jan 15, 2011
- Messages
- 13,119
Cyclist are notorious for using EPO. Track and field too. EPO is supposed to be a game changer in endurance sports....one wrong move and you are a dead man.
lol one injection of that and I may be a dead man
- Joined
- Jul 18, 2017
- Messages
- 1,723
So I was wondering whether EPO increased platelets and found this
Effects of erythropoietin on platelet reactivity and thrombopoiesis in humans | Blood Journal
"In summary, we showed that EPO markedly enhances platelet and endothelial activation in humans. Thus, we postulate that a patient-oriented approach to the use of EPO entails its administration not only to patients who are likely to respond to EPO but also to anemic patients, who additionally benefit from platelet activation. Whether heightened platelet reactivity and endothelial activation may increase the risk of thromboembolism warrants further investigation."
Here is another
https://www.ncbi.nlm.nih.gov/pubmed/10366799
"A 10% to 20% increase in platelet counts was observed in both EPO groups on day 5. In the placebo group, platelets increased only several days after the first phlebotomy."
So that is interesting because the vast majority of us on TRT/AAS generally do not seem to get increased platelets. So wouldn't that mean the mechanism IS different between TRT/AAS and taking EPO?? I am not sure we face the same risks those cyclists did.
From the study you posted:
In several animal species treatment with rHuEpo stimulated platelet production, but platelet counts tended to normalize after 1-2 weeks and large, chronic doses even caused thrombocytopenia.
AAS use is comparable to moderate chronic EPO stimulation, so that only moderate increases in platelet count are seen initially. And as stated above such increases in platelet count might only be temporary. Hence why we tend not to see elevated platelet counts in AAS users.In vivo data have shown that moderate Epo stimulation, i.e. that produced by standard doses of rHuEpo, short-term hypoxia or moderate iron deficiency, causes a moderate elevation of platelet counts, whereas intense Epo stimulation, as produced by high doses of rHuEpo, prolonged hypoxia or severe iron deficiency, causes some degree of thrombocytopenia. In the latter case, there appears to be a diphasic response to Epo, the initial positive response (a stimulation of platelet production) being followed by thrombocytopenia. Contrarily to the thrombocytopenia due to increased platelet destruction induced by other growth factors, Epo-induced thrombocytopenia is the result of an inhibition of platelet production.
- Joined
- Jan 15, 2011
- Messages
- 13,119
From the study you posted:
AAS use is comparable to moderate chronic EPO stimulation, so that only moderate increases in platelet count are seen initially. And as stated above such increases in platelet count might only be temporary. Hence why we tend not to see elevated platelet counts in AAS users.
Oh wow, I had no idea platelet levels increased the first 1-2 weeks when introducing TRT/AAS into our systems before normalizing. I guess no one really gets a CBC panel that early.
- Joined
- Jul 18, 2017
- Messages
- 1,723
I am just theorizing here, but I think a lot of that has to do with blood doping in general. When you ADD blood volume, it will automatically increase platelet count due to having more platelets. That is a primary risk for clotting. Combine that with a long ride and likely lower than optimal water levels due to excretion of bodily fluids through sweating, and you could compound the risk.
Just spit balling here, so I could be way off the mark.
https://en.wikipedia.org/wiki/Blood_dopingBlood transfusion begins by the withdrawal of 1 to 4 units of blood (1 unit = 450 ml of blood) several weeks before competition. The blood is centrifuged, the plasma components are immediately reinfused, and the corpuscular elements, principally red blood cells (RBCs), are stored refrigerated at 4 °C or frozen at −80 °C.[11] As blood stored by refrigeration displays a steady decline in the number of RBCs, a substantial percentage, up to 40%, of the stored RBCs may not be viable.[12] The freezing process, conversely, limits the aging of the cells, allowing the storage of the blood for up to 10 years with a 10% to 15% loss of RBCs.[13] Stored RBCs are then reinfused, usually 1 to 7 days before a high-endurance event.
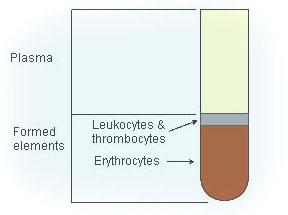
You can separate the leukocytes and platelets from the RBCs and only store and reinfuse the latter.
Stewie
Featured Member / Verified Customer
Featured Member
Kilo Klub Member
Registered
Verified Customer
- Joined
- Feb 3, 2011
- Messages
- 5,169
Could you briefly describe the 'Megalin receptor hypothesis'? Couldn't find much about it myself. Thanks!
Apparently they no longer exist in my bookmarks.
When Dat's board was up and accessible, there was a grad student (very brilliant young man) that went into exceptionally deep details of Megalin and Cubilin interrelationship with SHBG/internalization/diffusion of the AR. Unfortunately, that info no longer is available.
Then we have the newfound concept and I quote:
intramuscular androgen receptor content, but neither circulating nor intramuscular hormones (or the enzymes regulating their intramuscular production), influence skeletal muscle hypertrophy following RET in previously trained young men.
https://www.frontiersin.org/articles/10.3389/fphys.2018.01373/full
- Joined
- Jul 18, 2017
- Messages
- 1,723
Very cool stuff, thx Stewie. It's high on my reading list.Apparently they no longer exist in my bookmarks.
When Dat's board was up and accessible, there was a grad student (very brilliant young man) that went into exceptionally deep details of Megalin and Cubilin interrelationship with SHBG/internalization/diffusion of the AR. Unfortunately, that info no longer is available.
Then we have the newfound concept and I quote:
https://www.frontiersin.org/articles/10.3389/fphys.2018.01373/full
- Joined
- Mar 16, 2007
- Messages
- 25,912
I am just theorizing here, but I think a lot of that has to do with blood doping in general. When you ADD blood volume, it will automatically increase platelet count due to having more platelets. That is a primary risk for clotting. Combine that with a long ride and likely lower than optimal water levels due to excretion of bodily fluids through sweating, and you could compound the risk.
Just spit balling here, so I could be way off the mark.
Yeah, dehydration would really compound things. The problem is that some of them have died in their sleep, so probably not dehydration. In fact I have read that many of them set an alarm every few hours so they can get up and move around, with the hopes that the movement will discourage clots from forming.
Im not sure the % breakdown on deaths from using EPO vs blood transfusions.
Similar threads
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
oxandrolone
pct
peptides
quality raw
raw steroid powders
steroid cycle
steroids
suspension
sust300
sustanon
test
test 400
test ace
test cyp
test cypionate
test e
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren ace
trenbolone acetate
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
oxandrolone
pct
peptides
quality raw
raw steroid powders
steroid cycle
steroids
suspension
sust300
sustanon
test
test 400
test ace
test cyp
test cypionate
test e
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren ace
trenbolone acetate
Staff online
-
 Big AIFBB PRO/NPC JUDGE/Administrator
Big AIFBB PRO/NPC JUDGE/Administrator
Members online
- MAD_SCIENTIST
- danjb
- Steelsouth
- Unstopppable1
- Bloodtrail
- solarsentinel1
- control
- IntenseVolume
- waterman3676
- megroo
- MasteroniPepperoni
- Freedom69!
- Alsafir
- danieltx
- grammo13
- SpecialEd8256
- dieselbuilder
- need4tren
- oilyone03
- onyxmuscle
- 280
- aHarness
- joeyliftss
- Dx-Gainz
- btails
- MooseKnuckles
- Topgun12
- scum93
- richieid911
- NEMSZ
- trackstar19
- strongerlife
- Thick500
- Runner1032
- handinpants
- Alan1
- 360
- kastro
- Mysterio
- Muscle4fun
- TransAmWS6
- Elvia1023
- Big A
- MR. BMJ
- ALPHALIFEFITNESS
- NorwegianMuscle
- bfbjd617
- rubberring
- FastBunny
- _Strength_Specimen_
Total: 1,289 (members: 1,283, guests: 6)
Forum statistics























