Ferritin is a protein that involved in Fe (Iron) storage & release, and it is also (in addition to hemoglobin/haemoglobin [Hb], haematocrit [HCT], Fe, and other blood factors) lowered by phlebotomy (blood-letting).
Hb is a binding protein in erythrocytes (red blood cells) for O₂.
HCT reflects % of blood volume occupied by erythrocytes (RBCs): i.e., HCT ↔ Hb by the basic formula Hb (g/dL) * 3 ≈ HCT (%) [e.g., Hb of 15 g/dL ≈ HCT of 45%]
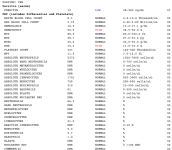
With respect to your question as to whether this means anemia -- anemia is defined as low HCT, and therefore low O₂ capacity (e.g., due to inadequate Fe intake) -- since your HCT is high, you are not anemic. Arguably, you are technically "iron deficient" otherwise called "iron deficiency anemia," but the consequence of that - low HCT - does not apply in your case thanks to androgen...
With respect to your bloodwork, this result is rather typical for TRT or androgen users that phlebotomize - your HCT is high, due to androgen (e.g., TRT) ↑HCT/Hb through an initial rise in EPO levels & a concurrent ↓Hepcidin levels (↑Fe uptake), which each fall back to baseline levels in response to ↑HCT/Hb (the new EPO/Hb set point). Your Fe & ferritin are low.
The decrease in your iron binding capacity (% saturation) follows from your low absolute Fe (iron) levels. Not likely from some obscure iron absorption problem.
The advice to take a break from frequent blood donation/phlebotomy makes sense, and the absolute risk for elevated Hb/HCT is not great - it's certainly worthwhile for (especially older men) androgen or TRT users to phlebotomize regularly (to lower Hb/HCT & thrombotic risks), but with less frequency (e.g., twice yearly).


































.gif "IP Gear")