
Ahh...that makes a lot of sense. Good info.No, but I would say that you can build an elite physique, as in win the Olympia, on anabolics & Met with everything else in place (including genetic endowment of course), because AMPK-mediated mTOR inhibition by Met is just not substantial enough to worry about with enough talent and proper drugs, nutrition, etc.

©ALL CONTENT OF THIS WEBSITE IS COPYRIGHTED AND CANNOT BE REPRODUCED WITHOUT THE ADMINISTRATORS CONSENT 2002-2024

























You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.







.gif "IP Gear")














What does metformin do exactly ?
- Thread starter fitnessmuscle
- Start date
- Joined
- Nov 27, 2009
- Messages
- 1,169
Warning. Old man rant coming …..
All of these cause an increase in mTOR:
-Cardio/Exercise
-Weight training
-Fasting
-Carbs
-Protein
-Leucine
I think all of this talk or worry about trying to manipulate it in some sort of favorable way or conversely; concern ourselves with various interventions to attempt to mitigate it - is all futile and borderline silly IMHO.
Some times we need to pan out, step back and keep it all in perspective; not only bc it’s sensible but for sanity.
Most of us do so many healthy things (exercise, nutraceuticals, food choices, quality sleep, keeping CVD and Diabetes and systemic inflammation risks low, etc) that absolutely support not only longevity and an anti-cancer state, but a healthy “health span” as well.
When we allow ourselves to get this granular, obsessed/paranoid, we are doing ourselves a serious disservice via additional unnecessary stress (cortisol release) thereby undoing the very thing we are trying to optimize (our health and longevity).
All of these cause an increase in mTOR:
-Cardio/Exercise
-Weight training
-Fasting
-Carbs
-Protein
-Leucine
I think all of this talk or worry about trying to manipulate it in some sort of favorable way or conversely; concern ourselves with various interventions to attempt to mitigate it - is all futile and borderline silly IMHO.
Some times we need to pan out, step back and keep it all in perspective; not only bc it’s sensible but for sanity.
Most of us do so many healthy things (exercise, nutraceuticals, food choices, quality sleep, keeping CVD and Diabetes and systemic inflammation risks low, etc) that absolutely support not only longevity and an anti-cancer state, but a healthy “health span” as well.
When we allow ourselves to get this granular, obsessed/paranoid, we are doing ourselves a serious disservice via additional unnecessary stress (cortisol release) thereby undoing the very thing we are trying to optimize (our health and longevity).
- Joined
- Apr 20, 2009
- Messages
- 6,795
Agree with this. Keep it simple, focus on what matters. I once knew a guy who told me he drove 45 minutes to the gym got there, realized he didn't have his intra shake, drive home to get it drove back.Warning. Old man rant coming …..
All of these cause an increase in mTOR:
-Cardio/Exercise
-Weight training
-Fasting
-Carbs
-Protein
-Leucine
I think all of this talk or worry about trying to manipulate it in some sort of favorable way or conversely; concern ourselves with various interventions to attempt to mitigate it - is all futile and borderline silly IMHO.
Some times we need to pan out, step back and keep it all in perspective; not only bc it’s sensible but for sanity.
Most of us do so many healthy things (exercise, nutraceuticals, food choices, quality sleep, keeping CVD and Diabetes and systemic inflammation risks low, etc) that absolutely support not only longevity and an anti-cancer state, but a healthy “health span” as well.
When we allow ourselves to get this granular, obsessed/paranoid, we are doing ourselves a serious disservice via additional unnecessary stress (cortisol release) thereby undoing the very thing we are trying to optimize (our health and longevity).
- Joined
- Nov 27, 2009
- Messages
- 1,169
Lol. Perfect example of insanityAgree with this. Keep it simple, focus on what matters. I once knew a guy who told me he drove 45 minutes to the gym got there, realized he didn't have his intra shake, drive home to get it drove back.
- Joined
- Sep 21, 2017
- Messages
- 646
Always solid fuckin answers!!Metformin is a biguanide, a class of drugs that aid in glucose disposal. Metformin decreases blood glucose levels by reduced gluconeogenesis (liver), decreased glucose absorption (intestines), and increasing insulin sensitivity (liver) by increasing glucose uptake and utilization.
While it seems a popular idea that Met increases skeletal muscle insulin sensitivity (which would be great for muscle anabolism), the primary site of its insulin sensitizing effects is the liver. Its actions on skeletal muscle is actually quite negative: it inhibits mTOR complex 1 (protein synthesis, translation) thereby reducing hypertrophy; it blocks the preferential shift from type I to type IIA fibers (resulting in a tendency towards reduced strength gains); and blocks the endurance training (LISS, HIIT, cardio) enhancement of insulin sensitivity. When Metformin alone is compared to a progressive resistance training program alone in older sedentary people, its effects (on blood glucose levels & absorption, insulin sensitivity) are indistinguishable from the resistance training program alone; and Metformin + progressive resistance training does worse than either Metformin with no training and/or resistance training alone.
Insulin (exogenous) promotes the uptake & utilization of glucose from the blood into skeletal muscle, repleting glycogen, enhancing insulin sensitivity in skeletal muscle. Rather than blunting fat synthesis & promoting fat oxidation like Metformin (another of Met's effects), it does the opposite potently, and dramatically increases VLDL synthesis in the liver (increasing the most dangerous particles for cardiovascular risks). Over time at high doses, it worsens insulin sensitivity by diminished autophosphorylation of the IR & its downstream elements, thereby reducing this skeletal muscle uptake of glucose and logically (though it has not been demonstrated insofar as I am aware) the muscle protein anabolic effects. See Insulin’s effects and mechanisms in promoting skeletal muscle hypertrophy, November 17, 2022, Type-IIx MesoRx Article
While the two drugs (Met & slin) may be used in diabetic patients, it requires dose reductions, and this is further complicated by AAS (that increase insulin sensitivity in skeletal muscle). Since slin so potently overwhelms the effects of Met and they act oppositely in some key ways, this should be considered before combining the two. A potential very high severity outcome is hypoglycemic shock, coma, and death.
- Joined
- Aug 31, 2015
- Messages
- 262
What dosage do u use?Anecdotal, so take it as you will, but for me metformin has:
Halved triglycerides
Lowered LDL
Increased pumps and fullness
Made it MUCH easier to stay lean
- Joined
- Sep 6, 2008
- Messages
- 3,307
500mg daily minimum.What dosage do u use?
I might move up to 1500mg if eating a lot of carbs.
- Joined
- May 19, 2004
- Messages
- 5,172
Good stuff as always.
How do we determine insulin sensitivity? When I began gh I started testing blood sugar in the am. It was always over 100. At home meter. But at doctor it was always perfect. All tests fasted. I began taking metformin it had no affect on these numbers. I'm thinking I have insulin resistance going on now.
I then got my a1c tested and find out it's actually low out of range. 4.3 then 4.7. this would indicate the opposite of what my hand glucose monitor says, that I'm very insulin sensitive, correct?
Is there a specific test that determines if we have good insulin sensitivity?
I'm a lazy SOB because I didn't bother to read closely enough to understand the protocol exactly, but it appears there is a way to test your insulin sensitivity that is commonly taugh to diabetics. As I understood it, it was basically based on how much 1iu of "fast acting" insulin lowers your BG. This could be done frequently as needed because sensitivity can change quickly.
If you can bother to do a quick google and digest the information perhaps you could explain it to me (us) in simple terms? Lol. I saw OTH did a reference to this test recently in some thread so perhaps he could chime in also.
I have some question regarding other natural insulin sensitizers/potentiators. I started reading bb mags in the early 90s and if any of you read Muscular Development you might remember some doctor who wrote columns there and was apparently on the Twinlab payroll and he was always talking about how chromium picolinate was actually a quite potent anabolic due to its interaction with the actions of insulin. I think he was referencing studies that showed lbm increases with chromium supplementation, but now I think they might have been misinterpreted, I don't know. As I remember Twinlab was putting 200mcg of chromium picolinate in pretty much ALL their supplements Lol. Recently I saw where Alex Kikel said to make insulin work quite a bit better you should take chromium every time you dose insulin. Kikel makes all types of wild claims Lol but as I was buying supps the other day I picked up a bottle of chromium too for a just a couple of bucks, can't hurt Lol. I wonder if it might be worth it to revisit lipoic acid as well as some kind of adjunct to insulin? Are there any other otc supps that might be good to take if using lots of insulin? Things like benfotiamine?
same for me here and i take a lot due to all the different health benefits.Anecdotal, so take it as you will, but for me metformin has:
Halved triglycerides
Lowered LDL
Increased pumps and fullness
Made it MUCH easier to stay lean
(currently 1g ER and 1g regular)
when taking combined with semaglutide, i drop Met to 500ER + 500reg and use 0,2mg semaglutide eod off-season
i would advise everyone to read this paper

Metformin and Its Benefits for Various Diseases
Metformin is a widely used biguanide drug due to its safety and low cost. It has been used for over 60 years to treat type 2 diabetes at the early stages because of its outstanding ability to decrease plasma glucose levels. Over time, different uses of ...
 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
i gladly sacrifice 1% muscle gain for the host of health benefits it offers
OuchThatHurts
Moderator / Psy, Ret.
Staff member
Moderator
Kilo Klub Member
Registered
Verified Customer
- Joined
- Nov 6, 2005
- Messages
- 10,523
Has anyone had any experience with Xigduo XR? It's an extended release version of two different types of GCAs. A SGLT2 inhibitor (dapagliflozin) and a biguanide (metformin). Seems to be both kidney and heart protective but there are no studies available that I can see other than the phase III clinical trial data. It was FDA approved and is sold in the US by AstraZeneca under the name Farxiga (dapagliflozin) and Xigduo XR (dapagliflozin + metformin).
Seems to be rather high (approx 1 in 10) in developing UTIs from the glycosuria which is part of a SGLT2's method of action.
Seems to be rather high (approx 1 in 10) in developing UTIs from the glycosuria which is part of a SGLT2's method of action.
- Joined
- Jul 30, 2006
- Messages
- 9,118
You can generally prevent or at least greatly limit by tapering up the dose. If I take a break and start back at 1000mg it will wreck my gut so I start at 250mg with last meal for 2-4 days then add a second dose with breakfast for 3-4 days then increase the night time dose to 500mg ER after a few days replace the late morning dose of 250mg to a 500mg ER.How no one has mentioned uncontrollably DIARRHEA is beyond me lol



- Joined
- Apr 20, 2009
- Messages
- 6,795
I think I've heard of that test. One time there was a lab error and my fasted BG came back at 35 they wanted to run it on me if a retest wasn't normal.I'm a lazy SOB because I didn't bother to read closely enough to understand the protocol exactly, but it appears there is a way to test your insulin sensitivity that is commonly taugh to diabetics. As I understood it, it was basically based on how much 1iu of "fast acting" insulin lowers your BG. This could be done frequently as needed because sensitivity can change quickly.
If you can bother to do a quick google and digest the information perhaps you could explain it to me (us) in simple terms? Lol. I saw OTH did a reference to this test recently in some thread so perhaps he could chime in also.
I have some question regarding other natural insulin sensitizers/potentiators. I started reading bb mags in the early 90s and if any of you read Muscular Development you might remember some doctor who wrote columns there and was apparently on the Twinlab payroll and he was always talking about how chromium picolinate was actually a quite potent anabolic due to its interaction with the actions of insulin. I think he was referencing studies that showed lbm increases with chromium supplementation, but now I think they might have been misinterpreted, I don't know. As I remember Twinlab was putting 200mcg of chromium picolinate in pretty much ALL their supplements Lol. Recently I saw where Alex Kikel said to make insulin work quite a bit better you should take chromium every time you dose insulin. Kikel makes all types of wild claims Lol but as I was buying supps the other day I picked up a bottle of chromium too for a just a couple of bucks, can't hurt Lol. I wonder if it might be worth it to revisit lipoic acid as well as some kind of adjunct to insulin? Are there any other otc supps that might be good to take if using lots of insulin? Things like benfotiamine?
I remember chromium and ala back in the day. I'd guess they help some but not like metformin
The high incident rate for side effects is mostly for women if you have a little deeper look into the studies. I took canagliflozin myself for over a year and had nothing. I know of other guys who take sglt2 inhibitors and they are fine too, when my girlfriend tried it she had an infection after 1 week of starting this medication. It's actually very rare for guys to have any sides.Seems to be rather high (approx 1 in 10) in developing UTIs from the glycosuria which is part of a SGLT2's method of action.
For insulin sensitivity I didnt feel like canagliflozin or dagaglioflozin did anything at all. It makes you pee out carbs. But if you are on a bulk and just shuffle in more carbs than before because you are taking that medication now then nothing will happen. So it has it's place imho but to me that is when I want to lose weight down rather than gain some.
OuchThatHurts
Moderator / Psy, Ret.
Staff member
Moderator
Kilo Klub Member
Registered
Verified Customer
- Joined
- Nov 6, 2005
- Messages
- 10,523
Okay. I can get that medication if I want from the doc. I only had a uti once inmy life many years ago and it sucked pretty bad. All I know is what the incidence was in the study. I didn't drill down into the study to see who got what and I'm not even sure if that data is even available. But yes, obviously women are more prone to these types of things than males but 1 in 10 seemed high as a group. And that was just my knee-jerk reaction. Did you have a deeper look into that study or was that just rhetorical on your part? You know of other guys, she wasn't, you didn't feel as though, in your opinion, etc, etc. See what I mean?The high incident rate for side effects is mostly for women if you have a little deeper look into the studies. I took canagliflozin myself for over a year and had nothing. I know of other guys who take sglt2 inhibitors and they are fine too, when my girlfriend tried it she had an infection after 1 week of starting this medication. It's actually very rare for guys to have any sides.
For insulin sensitivity I didnt feel like canagliflozin or dagaglioflozin did anything at all. It makes you pee out carbs. But if you are on a bulk and just shuffle in more carbs than before because you are taking that medication now then nothing will happen. So it has it's place imho but to me that is when I want to lose weight down rather than gain some.
What I know is that my doctor will prescribe this med, Xigduo XR, and if it's kidney, heart, and liver protective, I'm certainly all for that. My friend on here @Type-IIx (that's not a snitch tag) can maybe weigh in on this with some facts to go along with our experiences. He was the member IIRC that said SGLT-2 inhibitors > biguanides. So we have a sort of hierarchy of GCAs in terms of efficacy and modernity.
No I was actually dead serious.Did you have a deeper look into that study or was that just rhetorical on your part?
A good summary for benefits and sides:

Risks vs Benefits for SGLT2 Inhibitor Medications
Health care providers should carefully assess patients with diabetes mellitus before prescribing sodium-glucose cotransporter 2 inhibitor medications and monitor for adverse effects.
www.ncbi.nlm.nih.gov
Genitourinary Infections
About 10% to 15% of women taking SGLT2 inhibitor medications developed urinary tract infections and vulvovaginitis.26 This could be because of a glycosuria effect caused by SGLT2 inhibitors.27
Another good one:
The risk for urinary tract infections with sodium-glucose cotransporter 2 inhibitors: no longer a cause of concern?
Sodium–glucose co-transporter-2 (SGLT2) inhibitors improve cardiovascular and renal outcomes in patients with type 2 diabetes, including those with diabetic kidney disease. However, the US Food and Drug Administration and European Medicines Agency ...
www.ncbi.nlm.nih.gov
Overall, data from major outcome trials clearly suggest that SGLT2 inhibitors are not associated with an increased risk of UTIs [9–11]. The recent analysis from Dave et al. [19] added a set of real-world data pointing in the same direction. Observational studies including patients with a UTI history or specific populations (CKD, the elderly) are pieces of evidence that would advance our knowledge in the field. However, already existing data on the association of SGLT2 inhibitors with UTIs are largely reassuring and should enable more extended use of these drugs for the benefit of our patients.
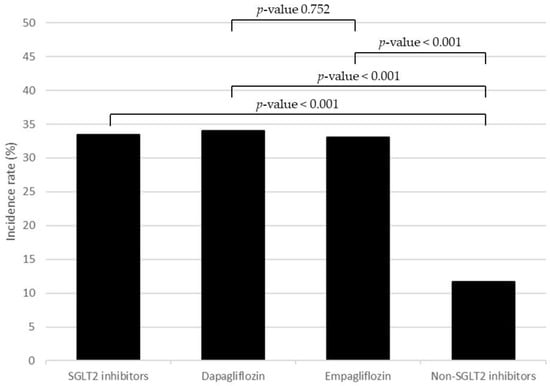
The Incidence and Risk Factors of Urinary Tract Infection in Patients with Type 2 Diabetes Mellitus Using SGLT2 Inhibitors: A Real-World Observational Study
Background: The incidence and risk of urinary tract infection (UTI) in patients with type 2 diabetes mellitus (T2DM) who use sodium glucose co-transporter-2 (SGLT2) inhibitors are still controversial. Therefore, this study aimed to investigate the incidence and risk factors of using SGLT2...
Conclusions: This study highlighted the high incidence of UTI in patients using dapagliflozin and empagliflozin compared with non-SGLT2 inhibitors. Additionally, patients of female gender and older age had a significantly higher risk of UTI when treated with SGLT2 inhibitors, whereas those with permanent jobs had a lower risk.
OuchThatHurts
Moderator / Psy, Ret.
Staff member
Moderator
Kilo Klub Member
Registered
Verified Customer
- Joined
- Nov 6, 2005
- Messages
- 10,523
It might be worth a try then. I do have an antibiotic on hand used (among other things) to treat UTIs so I'm fairly covered just in case. But if this could mean the difference between less pinning vs more, I'm 100% all for it.
- Joined
- Sep 27, 2018
- Messages
- 37
Anyone here talking the SHLTs
Similar threads
- Replies
- 58
- Views
- 2K
- Replies
- 22
- Views
- 639
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
oxandrolone
pct
peptides
quality raw
raw steroid powders
steroid cycle
steroids
suspension
sust300
sustanon
test
test 400
test ace
test cyp
test cypionate
test e
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren ace
trenbolone acetate
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
oxandrolone
pct
peptides
quality raw
raw steroid powders
steroid cycle
steroids
suspension
sust300
sustanon
test
test 400
test ace
test cyp
test cypionate
test e
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren ace
trenbolone acetate
Members online
- Brahma
- juiceball44
- badguy
- IFBBProDomCardone
- Ottovk
- MooseKnuckles
- Alan1
- jaysal555
- 22son
- hk55874
- musclehngry
- Sir Liftalot
- Yousef12O2
- chrisrivers
- Tristiand
- massd1213
- growing1221
- ryanfoster0
- TransAmWS6
- _Strength_Specimen_
- CorgisOnTren
- Heath82
- HughJass
- Onidus
- g.r.o.w.t.h.
- intensed
- Ranchhand
- 01dragonslayer
- btails
- northface384
- Freedom69!
- Kray
- mindyerinnards
- Hulk69
- Mute
- SABAGOY
- DamageInc
- bigorbust80
- Muay Thai
- Bigboycpt21
- vizzorz
- ZILLAMAN
- rpmgtr
- homonunculus
- IntenseVolume
- prototype5
- Misfit246
- trenathor
- TrippplePPP
- jdschio
Total: 1,314 (members: 1,307, guests: 7)
Forum statistics
- Total page views
- 561,224,923
- Threads
- 136,356
- Messages
- 2,784,642
- Members
- 160,552
- Latest member
- Connorarcher12























