
©ALL CONTENT OF THIS WEBSITE IS COPYRIGHTED AND CANNOT BE REPRODUCED WITHOUT THE ADMINISTRATORS CONSENT 2002-2024


























You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.







.gif "IP Gear")















HGH injection IM or Sub?
- Thread starter Dado5
- Start date
- Joined
- Dec 11, 2006
- Messages
- 34
sub
- Joined
- Jan 30, 2009
- Messages
- 2,816
Tried both. Didn't see a difference, so I stick with sub.
- Joined
- Dec 11, 2008
- Messages
- 1,437
Wow I thought there was virtually no diff IM or subq.
I thought the same. Actually my hormonal dr. told me that if you inject subq you loose some of it. And if you inject in to the muscle it will utilise all of it and release slowly.

Depends on Goals...
Dat has mentioned there is some evidence for sight specific growth when injected IM.
So, it depends on your goals a bit then- fat loss: SQ... muscle gain: IM.
One thought- IF the IM idea holds true, ultimately you SHOULD (other factor's involved obviously) eventually lose fat as well, i.e. more muscle, higher metabolism, more fat lost.
Dat has mentioned there is some evidence for sight specific growth when injected IM.
So, it depends on your goals a bit then- fat loss: SQ... muscle gain: IM.
One thought- IF the IM idea holds true, ultimately you SHOULD (other factor's involved obviously) eventually lose fat as well, i.e. more muscle, higher metabolism, more fat lost.
- Joined
- Jun 23, 2007
- Messages
- 75
answer
IM works best IMO
IM works best IMO
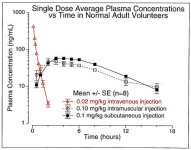
I attatched a chart showing the difference between sub-q and IM. Sub-q is better for fat loss.
So, the dosing used per kg/lbs was:
0.1 SQ
0.10 IM
0.02 I.V.
Translated -- IM inj's was just 10% of the reg. SQ dosing and for I.V. inj's, their dosing was a mere 2% of the SQ injs! That's hardly a fair comparison - but I've seen similar.
Note this study which compares SQ (SC), I.V. and I.N. inj's.
**broken link removed**
This other forum discussed how the I.V. injections were only a fraction of the normal SQ dosing to the above study.
**broken link removed**
My thoughts? If the above chart/study had of upped the dosages, we would have "WOW'ed at the results of the I.V. spike.
Note: Even at the current 2% dosage comparison to the SQ dose, the I.V. spike still exceeded 6x greater than the SQ. Further, if the I.M. were bumped up by a factor of 10. i.e. equal to the SQ dose, I.M (appears as if it too) would have greatly exceeded SQ inj.
Last edited:
Interesting. I should switch to sub-q
I don't know if were catching this here, but according to that chart, the I.M. dosage was a mere 10% of the SQ dose, yet the I.M spike lasted about the same duration as the SQ. Based on that alone, I.M. would be the better choice between those two, but not necessarily between the three.
By the way, I was PM'ed by someone who raised a point I too saw, but shrugged off as a misprint. The way the chart reads, 0.1 SQ and 0.10 I.M are protrayed as if they are different dosages, yet .1 and .10 are actually the same dose! However as the chart seems to suggest the dosages varied and I'm assumming (like other studies mostly do) SQ was the greater dose, I.M. second and I.V. the least.
It would certainly be nice to know whether or not the SQ and IM varied or not. Might I add, if there's no variation in dosage between these two, then SQ certainly appears to be the preferred choice.
Now depending on the misprint, I.V. was either only dosing 10% of the others or as little as only 2%. Either shows an incredible benefit for I.V. dosing. That is, I.V. spiked approx 6x greater at reduced dosage -- meaning if the I.V. dosage was raised, in theory, the I.V. spike/peak could have exceeded 60x to 600x greater, again, dependent on misprint! I know that seems far fetched, but it does seem appropriate. To explain -
Again, pay attention to the other study I gave links for which compared SQ (SC), I.V. and I.N. injections. It said,
"On the other two occasions the patients received an sc injection (0.10 IU/kg) and an iv injection (0.015 IU/kg) of GH, respectively."
Did you catch the difference in dosage? I.V. was only 1/8th of the SQ dose! However check out the spike/peaks!
"Intravenous administration produced a short-lived serum GH peak value of 128.12 ± 6.71 μg/l. Peak levels were 13.98±1.63 μg/l after sc injection "
I find that AMAZING and certainly useful. The I.V. just didn't double. i.e. increase 100%. Hell no! It increased approx 1000% above the SC dose.
Yeah, yeah, I know it's "a short-lived" spike/peak and according to the chart above and at the MINIMAL dosages we've seen so far, it seems we can expect (at minimum) a 2 hour window. However I keep thinking, what if we upped the dosages? How high the peak would really be? Would it stay true to the math? But more importantly, how long before it dropped back to base line? Again, we're dealing with minimal dosing.
Lastly, I know many in this forum dose as much as every 3 hours. If you were to implement I.V. into you routine, maybe splitting up your doses, i.e. 1/3rd IV and 2/3rds part SQ, you could experience the benefits of both worlds. You'd also confuse the body a tad as well via mixing up the dosing.
In the end, your dosing would be higher, your peaks would last longer, you'd mix up your protocol and use LESS because only minimal amounts are needed when dosing I.V.
I think you would need %100 pharm grade GH to shoot it IV. I'd be too scared to do that with generics. Even legit stuff like real hyges and riptropins,etc... couldnt the filler be harmful to shoot IV
I completely understand where you're comming from. However if you think about it, any GH (gen's or other) will eventually make its way the vascular wall and then on into your vein(s). Thus, whether you decide to fuel up directly into the vein or outside of it, rhGH at some point will make its way to the heart -- which is what I'm assuming you're concerned over?
Anyhow, don't be worried about admin techniques - unless done incorrectly, they're not what can hurt you, i.e. SQ, IM, IV, IN, etc. It's the substance that hurts and admin'ing bad or dirty GH via SQ, isn't gona spare you or your blood stream.
Last edited:
- Joined
- Jun 8, 2002
- Messages
- 4,917
So, the dosing used per kg/lbs was:
0.1 SQ
0.10 IM
0.02 I.V.
Translated -- IM inj's was just 10% of the reg. SQ dosing and for I.V. inj's, their dosing was a mere 2% of the SQ injs! That's hardly a fair comparison - but I've seen similar.
Note this study which compares SQ (SC), I.V. and I.N. inj's.
**broken link removed**
This other forum discussed how the I.V. injections were only a fraction of the normal SQ dosing to the above study.
**broken link removed**
My thoughts? If the above chart/study had of upped the dosages, we would have "WOW'ed at the results of the I.V. spike.
Note: Even at the current 2% dosage comparison to the SQ dose, the I.V. spike still exceeded 6x greater than the SQ. Further, if the I.M. were bumped up by a factor of 10. i.e. equal to the SQ dose, I.M (appears as if it too) would have greatly exceeded SQ inj.
0.1 and 0.10 are the same thing.....your thinking .01 vs. .1
0.1 and 0.10 are the same thing.....your thinking .01 vs. .1
Yeah, caught that too. Read my other post, 5 posts above - has other/better information regarding the findings.
I completely understand where you're comming from. However if you think about it, any GH (gen's or other) will eventually make its way the vascular wall and then on into your vein(s). Thus, whether you decide to fuel up directly into the vein or outside of it, rhGH at some point will make its way to the heart -- which is what I'm assuming you're concerned over?
Anyhow, don't be worried about admin techniques - unless done incorrectly, they're not what can hurt you, i.e. SQ, IM, IV, IN, etc. It's the substance that hurts and admin'ing bad or dirty GH via SQ, isn't gona spare you or your blood
The difference with IV and IV injections is the fillers or particals left behind after it turns to solution. This can build up in the walls of the veins in time. It's not an issue with im usage. Many iv drug addicts have had complications like endocarditis. Multiple IV use in the same veins will lead to a collapsed vein. Not to many drug users keep their vascularity for long. None of this is an issue thru muscling their drugs. Plus you might run the risk of getting tracks because the injections are not spread out as much as IM usage.
If anyone were to choose IV injections, you should always use a cotton filter to draw up your solution to minimize any particals that might be injected along with your HGH. Even Pharmecutial powdered morphine or with the finest China White which is the purist form of H, drug users filter their injections. Unless your HGH comes in a sterile liquid solution you should filter it. Not a cigarette filter either. You run an high risk of getting sick with a fever, cold sweats, and chills from the fibers (called cotton fever amongst drug users). A regular cotton ball should be used as a filter. Even though HGH powder is much finer than an average drug users injection of choice, It makes you think twice about doing IV injections doesn't.
BTW, this post makes it sound like I've been there, down that. Yes, at one time in my life.
The difference with IV and IV injections is the fillers or particals left behind after it turns to solution. This can build up in the walls of the veins in time. It's not an issue with im usage. Many iv drug addicts have had complications like endocarditis. Multiple IV use in the same veins will lead to a collapsed vein. Not to many drug users keep their vascularity for long. None of this is an issue thru muscling their drugs. Plus you might run the risk of getting tracks because the injections are not spread out as much as IM usage.
If anyone were to choose IV injections, you should always use a cotton filter to draw up your solution to minimize any particals that might be injected along with your HGH. Even Pharmecutial powdered morphine or with the finest China White which is the purist form of H, drug users filter their injections. Unless your HGH comes in a sterile liquid solution you should filter it. Not a cigarette filter either. You run an high risk of getting sick with a fever, cold sweats, and chills from the fibers (called cotton fever amongst drug users). A regular cotton ball should be used as a filter. Even though HGH powder is much finer than an average drug users injection of choice, It makes you think twice about doing IV injections doesn't.
BTW, this post makes it sound like I've been there, down that. Yes, at one time in my life.
Good points and I'll say if your GH has particals in it after recon, I'd be changing real quick to another supplier. Not because I'd be injecting IV, but because recon of GH should be crystal clear!
Course, as of late, I only use pharm grade and script -- so my experience over the last 6 months of IV usage consists only of those. The difference between IV and SQ/IM are easily felt.
I could have sworn Dat posted something a while back showing that IV was the worst way to use GH. I just have no clue where to begin searching.
Ah, that I would love to see. Yooo Dat??
With what I have read, peaks FAR exceed any other inj. type. However, yup - they're short lived and is why either frequent injections are required or dividing up (as I do) part IV & part SC works well.
There's also the supposed probability that IV does not stir/cause IGF-1 secretion as that one study stated. If so, then again, dividing the doses resolves that issue. Yet again, I keep saying that study (and another I've seen) only dosed IV at minimal amounts (1/8th in the above case) of the SC dosage. Thus my complaints are if you wish to do a fair comparison between anything, then use similar dosages for accuracy!
Similar threads
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
oxandrolone
pct
peptides
quality raw
raw steroid powders
steroid cycle
steroids
suspension
sust300
sustanon
test
test 400
test ace
test cyp
test cypionate
test e
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren ace
trenbolone acetate
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
oxandrolone
pct
peptides
quality raw
raw steroid powders
steroid cycle
steroids
suspension
sust300
sustanon
test
test 400
test ace
test cyp
test cypionate
test e
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren ace
trenbolone acetate
Staff online
-
 LATSModerator / FOUNDING Member / NPC Judge
LATSModerator / FOUNDING Member / NPC Judge
Members online
- airman
- raspberrypie
- LATS
- pyramid74
- QECon34144
- bigains
- danieltx
- 20sam91
- zman12
- Chipper Jones78
- gojimmgo
- taslajrisi
- Pull Freak
- Drax
- Khazad
- Mini Monster
- Seattlesbest
- Dot89051
- cm
- Samson250
- ALPHALIFEFITNESS
- 1234trew
- b-boy
- Xplicit
- TC
- ergo
- WeakFNG
- hevi-head
- badguy
- BIGEZ
- Idra
- Elvia1023
- Gunsmith
- derzwerg
- big_lech
- MDT
- aHarness
- grizzly978
- Bataille
- Onidus
- EricJ123
- Westen
- slesh
- Performance Based
- Hulk69
- Mufasa123
- rawtest
- deeganboy
- catta90ms
- freshsqueezed
Total: 1,332 (members: 1,324, guests: 8)
Forum statistics
- Total page views
- 559,684,662
- Threads
- 136,131
- Messages
- 2,780,563
- Members
- 160,448
- Latest member
- Jim311























