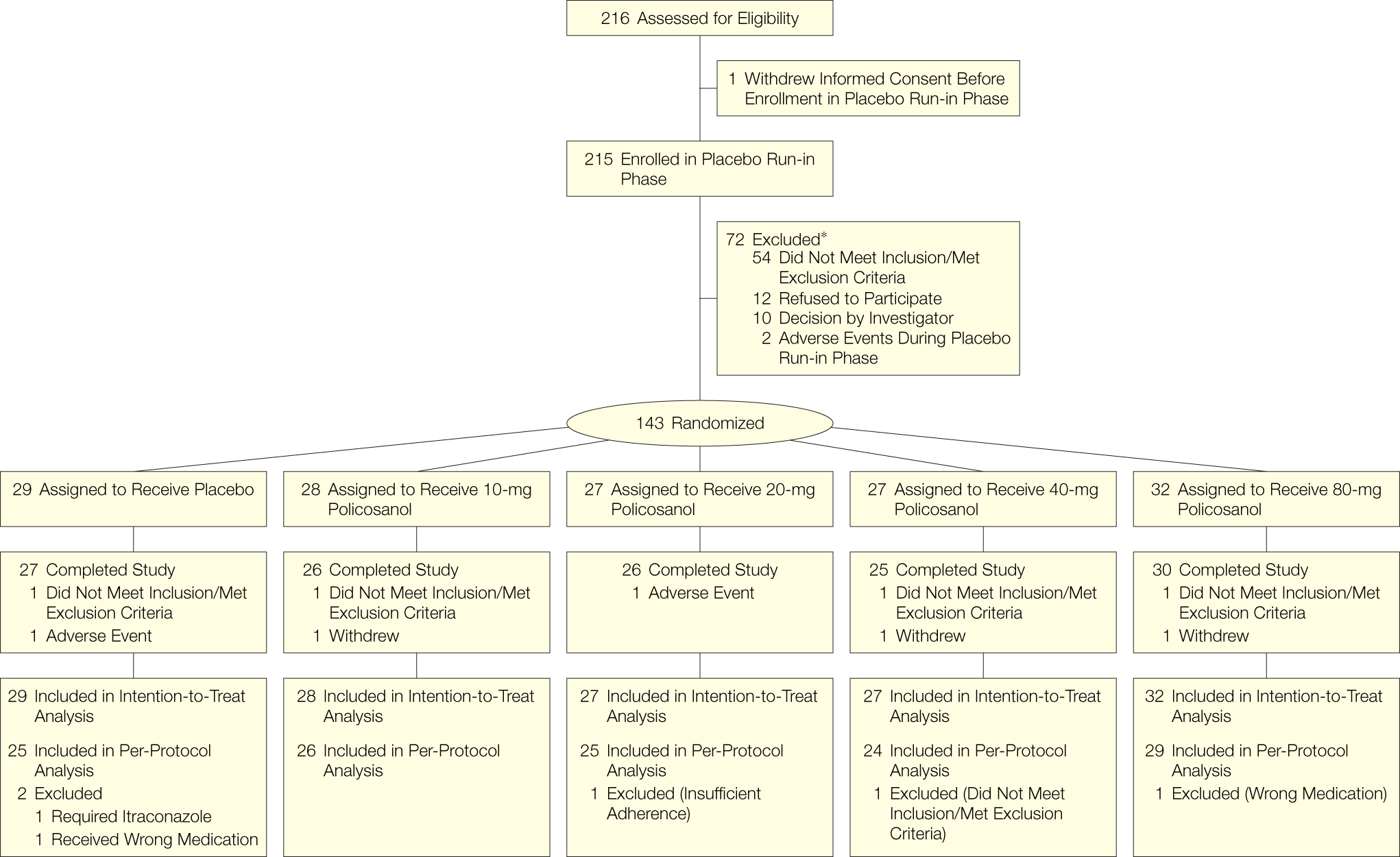
Our rigorously controlled trial found no effect of Cuban sugar cane–derived policosanol on lipoprotein levels in patients with hypercholesterolemia or combined hyperlipidemia beyond placebo. Our goal was to corroborate the effectiveness of policosanol in lowering lipoprotein concentrations and to determine, if effective, the dose-dependency of effects and optimal doses. Two of the 5 treatment groups were treated with usual doses (10 and 20 mg/d), while 2 groups received high doses (40 and 80 mg/d) of policosanol.
The study revealed no significant differences between the groups in all lipoprotein fractions examined, namely LDL-C, HDL-C, total cholesterol, VLDL-C, triglycerides, and lipoprotein(a). A nonparametric test (JT test) used to discover a possible dose-dependency as well as comparison of active treatment with placebo was not significant. The results are in contrast to a large number of published randomized controlled trials. Recently, a systematic review of the literature up to June 2003 of randomized controlled trials using policosanol was published.2 Concerning the primary end point of reduction of LDL-C, this meta-analysis found 29 eligible studies with 1528 patients receiving treatment compared with 1406 patients receiving placebo.
Twenty-eight of the 29 trials came from Cuba and 1 trial came from Argentina.15 Weighted estimates of percentage change in LDL-C were –23.7% for policosanol (mean dose of policosanol, 12 mg/d; range, 5-40 mg/d) vs –0.11% for placebo (P<.001). This LDL-C reduction is well in the order of magnitude that is achieved with commonly used doses of statins.16 In fact, some trials, again all but 1 from Cuba, directly compared the effects of policosanol with statins3,17-21 and found policosanol equally effective or better. Even a dose of policosanol as low as 2 mg/d was found to lower LDL-C significantly by more than 15%.22 It has been suggested that the lipid-lowering effects of policosanol are dose-dependent from 2 to 40 mg/d.23
The reasons for the discrepant results between our trial and previous studies are unclear. As nearly all previous studies have been performed in Latin America (1 positive study was performed in Russia),4 it cannot be excluded that either ethnic or nutritional factors contribute to the impressively potent lipid-lowering effects of policosanol reported. Although ethnic and nutritional differences between European white and Latin American patients might play a role, the magnitude of differences reported (no effect vs a consistent 25% LDL-C reduction) makes this explanation unlikely. Furthermore, other lipid-lowering drugs, such as statins24 and ezetimibe25 have been shown to have no ethnic-specific effects. The same holds true for responses to low-fat diet.26 Almost all studies were supported by 1 sponsor, Dalmer Laboratories, a commercial enterprise founded by the Center of Natural Products, National Center for Scientific Research, La Habana, Cuba, to market policosanol. Our group1 and other studies5,23 have therefore suggested that independent studies should be performed to prove the efficacy of policosanol. Until now, independently performed studies are scarce. Our trial is the first study to investigate sugar cane–derived policosanol independently from the aforementioned Cuban research group but still using Cuban policosanol. A randomized placebo-controlled trial from the Netherlands of 58 patients found no effects when using wheat germ policosanol (20 mg/d) on lipoproteins in patients with normal to mildly increased cholesterol.5
Very few other studies outside Cuba exist but are not convincing in quality. An animal study performed in Canada in hamsters showed that sugar cane and rice wax policosanol have no effects on lipids,27 which is in contrast with findings of a variety of animal studies from Cuba.28,29.
The putative mechanism of action of policosanol has not been clarified, although suppression of the 3-hydroxy-3-methylglutaryl coenzyme A reductase activity has been postulated.30 There are several possible limitations to our study. Our study design is generally accepted for studies investigating lipid-lowering agents and our trial was a multicenter trial. Lipid and lipoprotein measurements were obtained on 3 different days at baseline (pooled baseline) to get reliable values. The measurements were performed in a central, certified laboratory. The trial consisted of a placebo and diet run-in phase with instructions to adhere to a National Cholesterol Education Program step I diet,6 initiated 4 to 6 weeks before baseline values were drawn. Diet had no influence on the results, as confirmed by comparison of food diaries at the end of the run-in phase and the treatment phase. The treatment duration was 12 weeks. It might be argued that lipid-lowering effects take longer to develop, although currently no known pharmacological intervention would support this notion. In the meta-analysis of Chen et al,2 the average treatment duration of the 29 studies was 30 weeks and a mean LDL-C level decrease of 23.7% was found. Extracting the subset of the 12 studies that had treatment durations of 12 weeks or less, the LDL-C lowering effect in these trials was still 24%. Furthermore, the published positive policosanol studies found lipid-lowering effects already after 4 to 6 weeks of treatment.1 Moreover, the putative lipid-lowering effect of policosanol has been reported to plateau after 10 weeks of administration.29 We conclude therefore that trial duration cannot be made responsible for the observed absence of policosanol effects on lipids.
We used Cuban sugar cane–derived policosanol that was provided as bulk from Dalmer Laboratories; therefore, a difference in the source of policosanol as a reason for the discrepant results is highly unlikely.
Conclusion In patients with hypercholesterolemia or combined hyperlipidemia, the sugar cane–derived policosanol in usual and high doses does not demonstrate a reduction in lipid levels beyond placebo.


































.gif "IP Gear")