
©ALL CONTENT OF THIS WEBSITE IS COPYRIGHTED AND CANNOT BE REPRODUCED WITHOUT THE ADMINISTRATORS CONSENT 2002-2026

























You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.






















hgh IM injections
- Thread starter s.norman
- Start date
- Joined
- Jul 2, 2008
- Messages
- 138
The better question would be why would you want to?
I'm very sleepy, so I won't go into too much detail about this. The short answer is, "yes". But, I am with rhinofight on this one. Why would you want to? You can inject SQ, IM or even IV. SQ has the most desirable administration:longevity:activity profile as a whole, albeit not incredibly different than IM.
im alredi doin MTII inj SQ..too many inj in the same spot...its just as easy pinning pecs thats why i askedThe better question would be why would you want to?
can u do IM injections w/ hgh?
SQ less painful than IM, and w/simlar results. Thus, stick with SQ inj.'s.
Of course, I.V. beats either hands down with a peak/spike approx 600 x than either, and @ lower dosages at a mere 1/8th in size. Yes, that means you'll use less GH or $$$. Though spike durations last only 25% of the norm to the compared IM & SQ, this allows for administration up to every 2-3 hours IF you maintain a 1/8th comparable dosage.
Example: 4IU's delivered every 4 hours or 4 x daily (this is pushing some serious limits) via SQ = 16IU.
Or .5IU delivered every 2 hours or 8 x daily via I.V. = 4IU.
With the first, yeilding only 4 spikes totaling 16IU daily, and the latter offering 8 peaks which are approx 600X greater than either SQ/IM, my choice is simple.
What I've personally wound up doing was increasing all of my I.V. doses by a factor of 4. So instead of dosing .5,...dose 2IU. In theory, this also multiplies the GH peak duration equivalent to a reg. SQ/IM dose. Yeah OK, so how did I prove this out? I know, sometimes math or theories aren't enough.
 Let's just say, every time my peak is over, I come crashing down...and HARD. In other words, after I've concluded my morning routine, regardless if I've only been up for 6 hours, it doesn't matter! It's nite nite time for me 6 hours later. In other words, after my peak dies, so do I!
Let's just say, every time my peak is over, I come crashing down...and HARD. In other words, after I've concluded my morning routine, regardless if I've only been up for 6 hours, it doesn't matter! It's nite nite time for me 6 hours later. In other words, after my peak dies, so do I!If you wish to understand what these peaks feel like and what I'm trying to convey, TRY rhGH I.V. It'll be just another way to mix up your routines.
can u do IM injections w/ hgh?
yes you can. use you get an extra bonus injecting it Subq.
- Joined
- Jul 2, 2008
- Messages
- 138
SQ less painful than IM, and w/simlar results. Thus, stick with SQ inj.'s.
Of course, I.V. beats either hands down with a peak/spike approx 600 x than either, and @ lower dosages at a mere 1/8th in size. Yes, that means you'll use less GH or $$$. Though spike durations last only 25% of the norm to the compared IM & SQ, this allows for administration up to every 2-3 hours IF you maintain a 1/8th comparable dosage.
Example: 4IU's delivered every 4 hours or 4 x daily (this is pushing some serious limits) via SQ = 16IU.
Or .5IU delivered every 2 hours or 8 x daily via I.V. = 4IU.
With the first, yeilding only 4 spikes totaling 16IU daily, and the latter offering 8 peaks which are approx 600X greater than either SQ/IM, my choice is simple.
What I've personally wound up doing was increasing all of my I.V. doses by a factor of 4. So instead of dosing .5,...dose 2IU. In theory, this also multiplies the GH peak duration equivalent to a reg. SQ/IM dose. Yeah OK, so how did I prove this out? I know, sometimes math or theories aren't enough.
If you wish to understand what these peaks feel like and what I'm trying to convey, TRY rhGH I.V. It'll be just another way to mix up your routines.
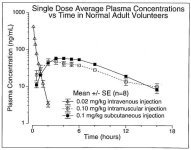
Wow, that's serious. I haven't reached that level of hardcore...yet. So, you say you crash along with the GH crash. What do you feel during the peak? 600x greater? I'm trying to picture that on a graph. Is that possible?
Although you have the site specific fatloss subq, personally i got better results IM in the delts. This was after years of trying diffierent sites and methods. As for the I.V. are you kidding?? No offense, but thats a little over the edge, no??
Wow, that's serious. I haven't reached that level of hardcore...yet. So, you say you crash along with the GH crash. What do you feel during the peak? 600x greater? I'm trying to picture that on a graph. Is that possible?
This is pretty much what he's referencing.
Attachments
SQ less painful than IM, and w/simlar results. Thus, stick with SQ inj.'s.
Of course, I.V. beats either hands down with a peak/spike approx 600 x than either, and @ lower dosages at a mere 1/8th in size. Yes, that means you'll use less GH or $$$. Though spike durations last only 25% of the norm to the compared IM & SQ, this allows for administration up to every 2-3 hours IF you maintain a 1/8th comparable dosage.
Example: 4IU's delivered every 4 hours or 4 x daily (this is pushing some serious limits) via SQ = 16IU.
Or .5IU delivered every 2 hours or 8 x daily via I.V. = 4IU.
With the first, yeilding only 4 spikes totaling 16IU daily, and the latter offering 8 peaks which are approx 600X greater than either SQ/IM, my choice is simple.
What I've personally wound up doing was increasing all of my I.V. doses by a factor of 4. So instead of dosing .5,...dose 2IU. In theory, this also multiplies the GH peak duration equivalent to a reg. SQ/IM dose. Yeah OK, so how did I prove this out? I know, sometimes math or theories aren't enough.
If you wish to understand what these peaks feel like and what I'm trying to convey, TRY rhGH I.V. It'll be just another way to mix up your routines.
123, I know you're a sharp guy, but I believe you might be over thinking this one. Of course your plasma levels of a drug/hormone/element/compound are going to reveal a greater "peak" from IV administration than plasma levels of the same things administered in some other way. If you pin one arm directly in the cephalic vein, then two minutes later draw blood from the cephalic vein in the other arm, of course your plasma GH levels are going to be off the charts. And, likewise, it's going to clear much, much faster than GH that is administered either IM or SQ.
It is better to have a lot of GH in our blood for several minutes, or a moderate amount of GH in our tissue for several hours? Obviously, the latter is desirable for any reason I can think of.
That study only added IV administration for the purpose of eliminating it as a viable delivery method. The reason they didn't use the same amount of GH in the IV study that they did in the SQ and IM studies is because they were using 27 ius of GH and the patient would most likely have had an adverse reaction to so much GH being pushed into their bloodstream at once.
Are you saying that you are tying-off and shooting up GH 4 to 8 times a day? I just don't see how that can be considered a healthy practice.
- Joined
- Mar 6, 2009
- Messages
- 30,459
I got better results for IM hgh injections. Sub Q made my hands numb.
If you pin one arm directly in the cephalic vein, then two minutes later draw blood from the cephalic vein in the other arm, of course your plasma GH levels are going to be off the charts. And, likewise, it's going to clear much, much faster than GH that is administered either IM or SQ.
The study is what it is,...and it clearly shows, regardless of testing methods, levels and durations of peaks. However to debate, since GH penetrates the vascular wall directly into the blood stream, isn't that the only logical place to draw testing from?
Though it's not just rhGH that requires reduced dosages when administering directly onto the vein/bloodstream -- everything (I can think of) admin'ed into the vein must be greatly reduced in dosage. And that's one of the benefits I was trying to point out, i.e. savings of!
It is better to have a lot of GH in our blood for several minutes, or a moderate amount of GH in our tissue for several hours? Obviously, the latter is desirable for any reason I can think of.
You're limiting the amount of times people in this forum pin. Hell, there's even some (though I think this is pushing it) wake up in the night and pin. However aside from them, I'd say more pin several times a day than those who admin only once. Again the added benefit -- If you pin multiple times a day, you could opt to inj. at least one of them via I.V. This assists with confusion, raises GH levels higher than you could obtain via mega dosing (blasting) AND all for less.
That study only added IV administration for the purpose of eliminating it as a viable delivery method.
That's an assumption without any proof. There's been many a study which utilized all delivery methods, i.e. IV., I.M., I.N., S.Q, etc. all in an attempt to determine which yeilded the best/favorable results.
Note this study which compares SQ (SC), I.V. and I.N. inj's.
**broken link removed**
It said,
"On the other two occasions the patients received an sc injection (0.10 IU/kg) and an iv injection (0.015 IU/kg) of GH, respectively."
Once again note the difference in dosage. I.V. was only 1/8th of the SQ dose! Now check out the spike/peaks!
"Intravenous administration produced a short-lived serum GH peak value of 128.12 ± 6.71 μg/l. Peak levels were 13.98±1.63 μg/l after sc injection "
Thus, the findings were similar in this other study, i.e. the I.V. just didn't double (increase 100%). Nope. Instead, it increased approx 1000% above the SQ/SC dose.
The reason they didn't use the same amount of GH in the IV study that they did in the SQ and IM studies is because they were using 27 ius of GH and the patient would most likely have had an adverse reaction to so much GH being pushed into their bloodstream at once.
- No kidding! I.V. does not require large or even normal dosing! Are you saying that you are tying-off and shooting up GH 4 to 8 times a day? I just don't see how that can be considered a healthy practice.
No I do not do that, but someone could. I'm telling you there's plenty in here already who dose 3-4 times daily.
Regardess of all, you're welcome to suggest the benefits are not worth the trouble. That's fine. However let me suggest -- once you've tried it, you'll never be able to deny the potency achieved and in all likelyhood, never remove it from your regimen (completely).
Wow, that's serious. I haven't reached that level of hardcore...yet. So, you say you crash along with the GH crash. What do you feel during the peak? 600x greater? I'm trying to picture that on a graph. Is that possible?
It's not "hardcore"
Though I wouldn't know how to describe it. Most is known about where or how high you've been, when you feel how fast and hard you're coming down. It's like clock-work. Depending on the dose admin'ed, depends on when you come down. For me, 1IU, about 4-5 hours later. 2IU, 6-7 hours later. Though I've not bothered, I would assume (the chart seems to suggest this) if I admin'ed .5IU, one would come down approx. 2 hours later, it's just I do not think you'd come down as hard -- due to the fact your peak wouldn't be as high.
Now Mega-dosing is hardcore. However even it, doesn't compare.
Regardess of all, you're welcome to suggest the benefits are not worth the trouble. That's fine. However let me suggest -- once you've tried it, you'll never be able to deny the potency achieved and in all likelyhood, never remove it from your regimen (completely).
This is exactly what I was saying...albeit in a nice way. IF there is any real benefit (not just speculation and feel), then how do we quantify it? REAL studies will need to be performed...blind at minimum...double blind preferably. The studies show that the GH rapidly clears the bloodstream. Which leads me to believe that the majority of it STAYS IN THE BLOODSTREAM and is filtered by the kidneys and doesn't migrate into the tissues.
I just don't see many people saddling up on the notion that you can save money and have GH spikes throughout the day just by pinning your veins a half dozen times a day (or even once or twice a day). Doing a SQ or IM injection is one thing. Tying off and lacing a needle into your vein is a very, very large and unsavory bridge that most people will not dare cross...especially for something that hasn't been proven to have any life-enhancing and/or tissue building benefits over the normal administration methods.
I don't want this to come across as anything other than what it is. Which is a modest disagreement between two like-minded, educated individuals. I believe that new ideas and hypotheses have to be questioned and not just taken at face value.
I do the things I do now for life enhancement purposes. I have worked out for over 20 years and have done some pretty large cycles, but those days are over. I am 42, 6'3", 225# and about 11% BF. My goals are pretty simple. I want to maintain a relatively low body fat level in the cold months and work down to 7%-9% in the warm months. I want to be healthy inside and out.
I am curious about you and your goals. Are you working for life enhancement or maximum muscular development?
Doing a SQ or IM injection is one thing. Tying off and lacing a needle into your vein is a very, very large and unsavory bridge that most people will not dare cross...especially for something that hasn't been proven to have any life-enhancing and/or tissue building benefits over the normal administration methods.
?
This was funny as hell. LOL
This is exactly what I was saying...albeit in a nice way. IF there is any real benefit (not just speculation and feel), then how do we quantify it?
Obviously studies. However yes, I'm able to gauge plenty from simple side effects. I've discussed this topic before in length. Certain side effects can even be used to gauge potency. In sum, side effects occur for a reason -- they're actually a "response to a cause". In other words, if you are receiving a side effect, something is causing it. Of course, one could be imagining those effects? If so, then thankfully YES we do have studies.
For instance, I've attempted to explain that by increasing the I.V. dosage, using a bit of math we can prolong/extend the GH peak duration comparable to that of SQ/IM, while achieving a peak value far greater than either SQ/IM is capable. Note the following study.
Plasma Clearance of Intravenously Administered Pituitary Human Growth Hormone
Journal of Clinical Endocrinology & Metabolism Vol. 60, No. 5 864-867
doi:10.1210/jcem-60-5-864
Copyright © 1985 by the Endocrine Society
"To determine at what rate the components are cleared from the circulation, blood was obtained at specific intervals following a bolus iv injection of pituitary hGH in hypopituitary patients. Each sample was gel filtered to determine its component profile of RIA values, which, when plotted vs. the time interval it represented, yielded a means of monitoring its disappearance from the plasma. Total hGH Was cleared with a t, of 21.5 min, the little component was cleared at 19.0 min, the big component was cleared at 26.5 min, and the pre-big component was cleared at 45 min. These data indicate that the larger the hGH component, the longer it takes to be cleared from the plasma."
To extrapolate from the study: In a nut shell, the higher the dosage, the longer the hGH component remains in circulation.
Thus, while I've stated I can literally feel the peaks and most certainly the crash, the above study confirms why I'm able to calculate their duration via dosage size. It's really not that complex a matter.
REAL studies will need to be performed...blind at minimum...double blind preferably. The studies show that the GH rapidly clears the bloodstream.
You're insinuating there may be benefits lost utilizing IV vs. SQ/IM? If so, note the following study (there are others).
Insulin-like growth factor-I response is comparable following intravenous and subcutaneous administration of growth hormone
Journal of Surgical Research, Volume 51, Issue 6, Pages 472-476
T. Kimbrough, S. Shernan, T. Ziegler, M. Scheltinga, D. Wilmore
"Subcutaneous (sq) administration of recombinant human growth hormone (r-hgh) has an anabolic effect and increases systemic insulin-like growth factor (IGF-I) in surgical patients. IGF-I is a mediator of growth hormone (gh) anabolic effects. To determine the effect of intravenous (iv) administration of r-hgh on systemic IGF-I, 11 patients were given 14 1-week courses of daily 8-hr infusions of r-hgh (10 mg in 500 ml D5W). Serum gh and IGF-I levels were measured. To compare routes of administration, iv r-hgh patients were matched to comparable sq r-hgh patients and IGF-I responses were examined. Illness severity effect on IGF-I response to r-hgh was assessed by dividing 16 burn patients who received either iv or sq r-hgh into two groups on the basis of severity scores. Analysis of the data showed that IGF-I levels increased significantly after iv r-hgh, IGF-I response to iv r-hgh (1.14 ± 0.18 U/ml to 4.12 ± 0.65 U/ml) was not different from IGF-I response to sq r-hgh (1.04 ± 0.36 U/ml to 4.96 ± 1.09 U/ml)."
Results? As far as IGF-1 goes (which is what we want secreted) = No difference!
So as far as studies go, this is where you're losing me. Yes, durations are shorter as most studies utilized smaller comparable dosages. Yet this is countered via implementing larger doses. GH I.V. administration has been around from rhGH conception. It, along with other forms of administration have been researched and even exhausted. Many of the studies (I could cite 10 right now) which addressed and tackled your very concerns. For instance, you said,..
I just don't see many people saddling up on the notion that you can save money and have GH spikes throughout the day just by pinning your veins a half dozen times a day (or even once or twice a day).
First off, let's be clear before I continue. DON'T pin "half a dozen times a day"! However once or twice a day? Yeah, I believe I said, "you could opt to inj. at least one of them via I.V." Meaning, try one IV a day. Not necessarily multiple times, though I did say, "but someone could." Thus, the option. Personally, I feel once is enough, though studies have been clear to point out, two and even more times are better. Again, note the following study.
Time Mode of Growth Hormone (GH) Entry into the Bloodstream and Steady-State Plasma GH Concentrations, Rather Than Sex, Estradiol, or Menstrual Cycle Stage, Primarily Determine the GH Elimination Rate in Healthy Young Women and Men
The Journal of Clinical Endocrinology & Metabolism Vol. 84, No. 8 2862-2869
Copyright © 1999 by The Endocrine Society
"Endogenous GH half-lives presumably represent pseudosteady state values, because GH is secreted episodically in short term bursts akin to consecutive brief IV infusions with resultant plasma levels (especially during the night) that do not decay to zero before additional GH release occurs."
Did you catch that? According to this study, consecutive, i.e. multiple IV infusions better mimics our naturally secreted GH algorithms due to the brief intervals IV is capable of.
Further they stated,
"We thus conclude that for any given body surface area, the elimination properties of GH in men and women reflect predominantly the time mode of hormone entry into the circulation, rather than gender, menstrual cycle stage, or prevailing serum estradiol concentration.....The time mode of entry of GH into the bloodstream significantly governs the determinable half-life of GH removal"
In other words, they determined the amount given throughout the day, i.e. intervals and that once born into the bloodstream are what determined the GH half-life and its clearance rather than any other supposed (mentioned) factor or variable.
Doing a SQ or IM injection is one thing. Tying off and lacing a needle into your vein is a very, very large and unsavory bridge that most people will not dare cross...
There are a few legit reasons not to try IV. However I contest they are not based on a lack of research or unfamiliarity. Yet injecting via IV is not as bad as most "fear". For myself, I do not tie off. My vascularity is desirable and dosages are so small, it's pointless. None the less, if anyone has any concerns and or does not know what they are doing, then don't.
I don't want this to come across as anything other than what it is. Which is a modest disagreement between two like-minded, educated individuals. I believe that new ideas and hypotheses have to be questioned and not just taken at face value.
Acknowledged.
I am curious about you and your goals. Are you working for life enhancement or maximum muscular development?
I'm 46. It's been a long haul, yet I'm out for and have been achieving both without extremes to either. That is of course, unless IV dosing is extreme?
I can only imagine where this would have went if I had mentioned the coagulation of an IV dose in addition to a SQ.
Or have I already? - Joined
- Jul 21, 2002
- Messages
- 11,596
can u do IM injections w/ hgh?
If I'm injecting PWO I always inject IM.
- Joined
- Oct 27, 2009
- Messages
- 260
If I'm injecting PWO I always inject IM.
Same here... Otherwise its sub-q in the abs
Similar threads
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
dragon pharma
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
pct
peptide
peptide suggestions
peptides
steroid cycle
steroids
suspension
sustanon
test
test 400
test cyp
test cypionate
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren
tren ace
tren ace buy
trenbolone acetate
winstrol
Popular tags
aas
aas testing
anabolic steroids
anabolics online
anabolid steroids
anadrol
anadrol drol tabs inj
anavar
anavar and winnie
body building
body building supplements
bodybuilder
bodybuilding
bodybuilding steroid test
clenbuterol
cycle
deca tren dosage
deca-durobolin
dianabol
dianabol and oxy
dragon pharma
gear
hcg
hgh
motivation
muscle building
muscle mass
nandrolone
pct
peptide
peptide suggestions
peptides
steroid cycle
steroids
suspension
sustanon
test
test 400
test cyp
test cypionate
test prop
testosterone
testosterone boosters
testosterone cypionate
testsuspension
tren
tren ace
tren ace buy
trenbolone acetate
winstrol
Members online
- Bigdog727
- artie farkalarty
- geno9
- Karađorđe
- BI22069
- WeakFNG
- Bigmac7486
- pesty4077
- bigchuck
- claymore
- Jewsy
- Thisiswhoiam
- gomcapt
- Facefactor
- staatz12
- RRBRRJ
- TheOtherOne55
- remmy
- theo
- KyleSmith1985
- musclemuscle
- cm
- DeeSol
- turbotaone
- Canuck54
- 8a
- JD2JR
- Nate Dawg
- ERock5
- seventhlttd
- Lily.
- ALPHALIFEFITNESS
- iam2big4me
- Virtues
- nothuman
- Sammy_J
- Squat to death
- Big A
- 01dragonslayer
- naps_for_gains
- Alan1
- Cinder
- Vr6chop
- solarsentinel1
- hawkmoon
- Palifter
- AMERICAN SUPPLY
- hrhnick
- xpac2
- Ber_tren
Total: 1,580 (members: 1,570, guests: 10)
Forum statistics
- Total page views
- 640,180,438
- Threads
- 142,654
- Messages
- 2,961,201
- Members
- 183,003
- Latest member
- harryhsm























