- Joined
- Dec 22, 2007
- Messages
- 8,190
Was the 1iu taken post-training?
By thyreocomd, do you mean t3 or t4?
t3 and t4 formula. Levothyroxine and Liothyronine

































.gif "IP Gear")















Was the 1iu taken post-training?
By thyreocomd, do you mean t3 or t4?
Emeric, are you sure its not 10iu? 1iu will do absolutely nothing, and e3d? Makes no sense at all. What type of insulin are they using? Even if it was long acting, like Lantus, you'd still need a much higher dose. They might be breaking records but that doesn't mean it's from the slin. The protocol basskiller laid out at his site years ago, believe it's called mutants protocol or something, is spot on in my opinion. Slin and gh pre, with lr3 post. They had it right, and all the new data still points in that direction. We are trying to maximize muscle mass, that's why around training is perfect timing in my opinion.
OJ and slin 3-4x a day, sure will put on mass but not good mass for a guy like me. I don't even drink juices with all that sugar. Why use juice sugars when you can use a quality carb? This is exactly what Dave is complaining about lol guys just taking slin to put mass on, any mass....
 I am all for being smart with drug intake and getting guys to use the smallest dose possible. But 1IU every 3 days is a complete joke. Yes it will do something but in the grand scheme it's nothing... you might as well give them the OJ instead. As MA highlighted we produce that amount naturally all the time. I wonder how much aas these Russian weightlifters were on too. Emeric I love your posts but you are not going to convince me these guys breaking world records (Russia has been in trouble many times for drugging up athletes) were on 1IU slin every 3 days with 20mg test and 5mg tbol every 3 days. Although I am sure many drug cheats did/do use small amounts thinking it will give them an edge without being too obvious.
I am all for being smart with drug intake and getting guys to use the smallest dose possible. But 1IU every 3 days is a complete joke. Yes it will do something but in the grand scheme it's nothing... you might as well give them the OJ instead. As MA highlighted we produce that amount naturally all the time. I wonder how much aas these Russian weightlifters were on too. Emeric I love your posts but you are not going to convince me these guys breaking world records (Russia has been in trouble many times for drugging up athletes) were on 1IU slin every 3 days with 20mg test and 5mg tbol every 3 days. Although I am sure many drug cheats did/do use small amounts thinking it will give them an edge without being too obvious.No is not 10IU, is no any study backing up this 10 IU ? I don`t go by this mutant protocol.
The range of the Russian pharmacological studies was very wide.
Sport pharmacology is not acknowledged in the USA.
This pharmacologic techniques was use to improve recovery from heavy
training, without causing any negative side effects or damage.
Heavy preparatory training in the resistance developing stage of adaptation can suppress insulin and thyroid activity. This weight lifter were training 2 times per day 3 day per week. They were supplemented in a dose 1 IU per 70 kg body weight every third day, and thyreocomd 20 -50 micrograms a day for 20 days cycle.
Is not my business of how much insulin some bodybuilder use, just sharing some healthy information and I don`t want get in to any argument.
Perhaps Russian slin is 10x stronger
Just a discussion brother, no argument. I was just asking cuz it peaked my interest that they would do such a thing, doesn't seem optimal at all. But if you do look at some of that stuff, like you hinted to, it's unorthodox compared to what we see these days.
Thanks for sharing.
Are you referring to off-season bodybuilders, or pre-contest...because there's a BIG difference between the two. Like I said above, I DO believe visceral fat is a factor in off-season bodybuilders; particularly the ones with insulin resistance. However, I think it's FAR less of a problem in contest ready bodybuilders. Visceral fat is the first fat to be lost when someone starts dieting, so it doesn't make sense that a large amount of it would till be hanging around by the time they hit 3% BF. In order for this to happen they would have to be carrying a LOT of visceral fat to begin with--far more than normal. Furthermore, insulin sensitivity tends to improve greatly during contest prep (which will also help reduce visceral fat), so by the time they hit the stage their insulin sensitivity is usually way better than it was during the off-season.
I like your post, but I take issue with the "percentages", as almost EVERY case of distension in bodybuilders is multi-factorial...and visceral fat usually isn't the most significant factor. Anyone who has been around high-level bodybuilders for a while knows that there are often MANY factors involved in distension, especially during the off-season when food intake is high and insulin resistance is more likely to occur.
For example, food intake is, in my opinion, the #1 cause of off-season distension in bodybuilders. The evidence for this takes place every day. You see, most of these guys wake up in the morning with a flat or near flat stomach, and by evening...or even mid-day...they look like they are well into their 2nd trimester. I've experienced it in myself and I have seen it happen in literally hundred's of others. Just go ask these guys what happens to their stomach as the day goes on. The vast majority will tell you that food intake is without any doubt a huge factor in distension....and the proof comes every day as we watch the stomach balloon further outward with each successive meal.
This isn't as big of an issue for the smaller guys, but for the bigger guys who need to push large amounts of food daily, it is a MAJOR (the most significant) cause of distension during the off-season. This is undeniable and anyone who denies it is completely inexperienced when it comes to high-level bodybuilders and the effect diet can have on the midsection. Since our level of visceral fat doesn't change throughout the day, food intake is the only logical explanation for why so many guys start out with a flat stomach in the morning and end up with a turtle shell by nightfall.
There are many other factors involved as well, at least 6-8 common ones, that take place in bodybuilders to varying degrees. Most bodybuilders are experiencing several of them simultaneously...and when combined with massive food intake, it is going to result in significant distension.
Interesting observations, though. I would assume that of the bodybuilders you've seen who did have significant visceral fat build-up, they probably had pretty bad insulin resistance as a result of abusing GH and insulin (and possibly a less than ideal diet).
Perhaps Russian slin is 10x stronger
Drug Test Anal. 2016 Oct 10. doi: 10.1002/dta.2110. [Epub ahead of print]
Potential detection of low-dose transdermal testosterone administration in blood, urine and saliva.
Schönfelder M1,2, Hofmann H3, Schulz T3, Engl T3, Kemper D3, Mayr B4, Rautenberg C5, Oberhoffer R3, Thieme D5.
Author information
Abstract
Administration of low amounts of endogenous hormones - so called micro-dosages - are supposed to represent a major challenge in doping analysis. To model such a situation, we have studied transdermal administrations of 2.4 mg/24 h testosterone patches and examined various steroid concentrations in blood, urine and saliva of 11 volunteers. Multiple samples were collected at t = 0, 3, 6, 9, 24, 48 and 72 h in four different phases, i.e. all combinations with/without physical exercise and with/without testosterone. Testosterone was analyzed by enzyme-linked-immuno-assay as well as by mass spectrometry in validated in an accredited anti-doping laboratory. Circadian controls with and without exercise did not provoke prominent alterations of whole, free, and salivary testosterone. Testosterone application for 24 h led to a significant (all p < 0.001) mean increase above controls: total testosterone (median: 5.2 vs. 8.0 ng/ml), free testosterone (median: 11.3 vs. 15.6 pg/ml), and salivary testosterone (median: 62.4 vs. 99.9 pg/ml). Additionally, all three testosterone measurements indicated significant correlations to each other (all r > 0.538, all p < .001). Circadian-matching showed peaking testosterone values after 6 h and 9 h, reaching highest augmentation up to 252.6 ± 123.5% in saliva after 9 h. After removal of testosterone patch, all testosterone levels in blood, saliva, and urine returned to baseline within 24 h. Different techniques of hormone detection (ELISA, GC-MS/MS, LC-MS/MS) indicated significant correlations. Results indicate that saliva, blood, and urine exhibit comparable hormone augmentation during micro-dose testosterone application, indicating a possible consideration in future doping analysis. The inter-individual variability was high in all biofluids, requiring the use of individual biological passport rather than statistical values.
Regarding low dosages of drugs in athletes, one doping method involves using something like 2mg of testosterone via transdermal application. The dose is so small it raises no flags on drug tests. Microdosing. Effectiveness for athletes: questionable. Effectiveness for bodybuilders: zero. You have to put the info in the proper context, what are you trying to achieve? Same as with the insulin.
Even 5mg test or tren or whatever can make a small difference but let's be real here. Sometimes I wonder if you really believe the stuff you write regarding dosages. I see you have mentioned Tony Freeman a few times recently how he will be on 140mg test and then move down to 70-80mg. I know you have mentioned a lot in the past how that system ensures health and progress can still be made. If he has to lose 40 pounds like he does then it could be a possibility. But do you honestly think a guy like that uses anything like that when competing at 280 pounds on stage at the O? Do you think he will honestly run that when stepping on stage at the Masters O? I am far from thinking everyone uses high doses (far from it) and I agree bodybuilding has become ridiculous drug wise but let's be real here. If you said to me Tony will be on about 800mg total of aas (test, tren, mast, winny etc) to compete at 245 pounds at the Masters O I wouldn't doubt it... but 140mg test at his highest?
Toney sitting at 280 on HRT is completely irrelevant without providing context. Many of us have seen advanced bodybuilders go off everything, not even training at all, and maintain an impressive amount of size for a few months. Does this mean you don't need any drugs at all to get to a certain size? Of course not. It's all about context. Let's say Toney was doing 3 grams and 12iu gh plus cycling insulin at his biggest he is going to need even more if attempting to surpass that. 140mg of test and 1iu insulin is going to do jack shit if more size is the goal. Now losing 40lbs to go into the physique division is another matter. Context. Like Rex Feral once said, if I remember correctly, if you aren't prepared to do 1000-1500mg of just test (not counting the rest) forget about national level bodybuilding. So when emeric comes in and recommends 30mg to an aspiring bb looking to compete at that level makes no sense. Now if he was talking about health primarily then that's something else, but he isn't providing the proper context.
Well, I respect your opinion. But yes you will notice the difference. This protocol was used by Soviet and East Germany national weight lifting team members.
Many of the leading sports scientists and coaches from the former Soviet Union, East Germany, Hungary, Bulgaria and Romania was and still using this protocol.
Also Victor Conte used a similar protocol with great results.
You need to try it out.
I am referring to guys who have very low subq fat, a great deal of muscle bulk and are below 10%.
Some level of distension is due to food in the GI tract ( not stomach..) but thats easy to tell..you can easily see distended loops of bowel.. again..im not guessing when i say this. I am very open about when i am sure of something or when im just spitballing. I can VERY easily see if it was food.
OK..right now if i just ate a ton of food yes my abdomen would protrude a bit but that is not what i am referring to.
Please look up MRI in and out of phase imaging as well as fat sat. I dont know how to be more clear...its is FAT. Its fat signal as clearly drops out, its BETWEEN loops of bowel... im just reiterating the same thing but you get my point.
As i said above most of the time, a large % of the time there is not diastastis of the rectus but there is visceral fat protrusion, the other part of the time there is diastastis along with visceral fat accumulation and a small % of the time its due to most commonly liver enlargement along with visceral fat to a lesser degree.
If you have any friends who have this just slap an ultrasound probe on them as I have done to my friends. It is quite clear. Or even an x ray will show u to some degree.
I have seen guys reverse it thought but its incredibly challenging without losing muscle mass. A guy at my gym back in NY came for abdominal pain and they found a pancreatic lesion ( turned out to be a cyst but you cant come down hard on CT) so he got an MRI. I read the MRI and let him know he would live but would need follow up. He dropped a ton of weight ( like 50+lbs) over the next 6months and on his follow up scan had no abdominal protrusion and barely any visceral fat. Once he learned it really was just a cyst he went back on gear. He looked amazing with a small waist and gained back like 30lbs. Just an example though. It can be lost its just very challenging hence i mentioned a few ways which may help.
Guys i dont have all the answers why a combo of maybe androgens, overeating, GH and insulin and its different effects on visceral vs subq and then stretching the abdominal wall and internal pressures and then for a combo of reasons you dont lose the visceral fat at the same pace as subq etc etc. but i am certain that for the cases i have seen which is quite a few that accumulation of visceral fat was causing internal mass effect and was greatly contributing to the abdominal distension. I could see if there was food in the GI tract, i could see if rectus was torn, i could see if organs were enlarged... most people reading the study wouldnt even be looking for that stuff but outside of my day job i love BBing so i try to learn more and disseminate as much factual info as possible. Together we can then learn to prevent and if needed combat it.
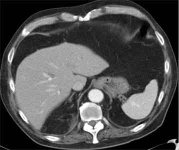
This is NOT my personal patients images. It is only an image i found online. This isnt even a bodybuilder! There is still too much subq fat but this person isnt "fat" but look at all the visceral. Imagine the same thing but with barely any subq fat and a lot more visceral fat.
On this image there are inches of fat between liver and rectus. And as you can see by lack of muscle bulk this wasnt even a bodybuilder so I doubt they were consuming insane amounts of food plus GH and insulin etc. THis is just someone "normal".
This is just to illustrate as some people were confused what visceral fat even was.
This days bodybuilding is out of control.
I have Tonny Freman on 140mg test per week for 8 weeks and 600mg per day one of my supplement, he is 280 lbs with only 3 meals per day. He will come down to 70mg per week for 6 weeks than back to 140 mg per week. He changed his mind and he will come back to compete, next year in the classic category at 245 lbs.
I read about the 1iu Russian protocol. It wasn't taken in an environment with other bodybuilding drugs like high steroids and gh and not for muscle gain either. The interesting thing is that the Russian and DDR athletes were buying extra steroids on the black market to add to the prescribed protocol. That's why they did the dbol/cortisol test, to see if the athlete was abusing drugs.
Emeric saying Milos protocol is "wrong" is ridiculous... yes it's wrong if you are an 150lb athlete not wanting to gain a single pound, just trying to correct some perceived or speculated "underproduction". I also remember the Russian plan called for small doses of opiates after particularly hard sessions for "recovery".
I feel Emerics posts are frequently ridiculous, they don't apply at all to what is actually being discussed.